
advertise here
Original Article
Role of hypothyroidism in dyslipidemia and blood glucose regulation.
Year : 2019 | Volume : 7 | Issue : 2 Page : 56-61
Context:
Overt hypothyroidism is an established risk factor for insulin resistance and hyperlipidemia Aims: To evaluate the role of thyroid dysfunction on alteration of glucose and lipid metabolism leading to insulin resistance, an important risk factor for cardio vascular diseases. Setting and Design: In this study we included 50 subjects, aged 25 to 35 years. This is a case control study conducted in department of Biochemistry. Materials & Methods: Investigations like fasting and post prandial blood sugar, HbA1c and lipid profile (Cholesterol, Triglycerides, HDL, LDL & VLDL) were done. Blood pressure was measured. Body weight and height were measured and BMI was calculated. All the parameters were analyzed using XL 640 fully automated random access analyzer. Statistical analysis used: tudent t test was used using graph pad quickcalcs software.
Results:
The cases were selected based on T4 and TSH concentrations whose values were significantly decreased and elevated respectively. The patients with hypothyroidism exhibited significant increase in concentration of total cholesterol, LDL, fasting blood glucose and HbA1c while HDL (p<0.05) showed a decrease in its concentration in comparison to controls. BMI and diastolic blood pressure showed significant elevation in hypothyroid individuals when compared to controls.
Conclusions:
It is evident from this study that insulin resistance bears an indispensable role in connecting T2DM and thyroid dysfunction. Cardiovascular events are the counter reflection of resurgence of heavily disturbed lipid metabolism due to thyroid dyscrasias.
Keywords: Hypothyroidism, lipid profile, glycated hemoglobin, blood pressure and BMI
Key Messages:
Careful screening of patients with hypothyroidism is necessary to determine the lipid and diabetic status with the aim of timely treatment and prevention of the development of atherosclerosis and potential complications of atherosclerosis.
INTRODUCTION
Hypothyroidism is defined as a deficiency of thyroid activity. It results from reduced secretion of total thyroxine (T4) and triiodothyronin (T3). Hypothyroidism is a clinical syndrome due to deficiency of thyroid hormones which results in a generalized slowing down of metabolic process.1. Overt hypothyroidism is an established risk factor for insulin resistance and hyperlipidemia.2 Hyperlipidemia is one of the components of metabolic syndrome. In some studies, metabolic syndrome and its components (dyslipidemia) are responsible for 25%of the new onset cardiovascular disease (CVD).3 Thyroid hormones have an important regulatory effect on glucose and lipid metabolism, and blood pressure control.4
In iodine-replete areas, most persons with thyroid disorders have autoimmune disease, ranging from primary atrophic hypothyroidism, Hashimoto’s thyroiditis to thyrotoxicosis caused by Graves’ disease.5 Thyroid hormone action has long been recognized as an important determinant of glucose homeostasis.6 The role of hyperthyroidism in diabetes was investigated in 1927, by Coller and Huggins proving the association of hyperthyroidism and worsening of diabetes. It was shown that surgical removal of parts of thyroid gland had an ameliorative effect on the restoration of glucose tolerance in hyperthyroid patients suffering from coexisting diabetes.7
There is recent trend in cardiovascular sciences towards assessment of thyroid function in cardiac conditions as there is relation in between thyroid function and lipid metabolism which is risk factor for cardiac disease.we try to confirm this relationship with biochemical assays.

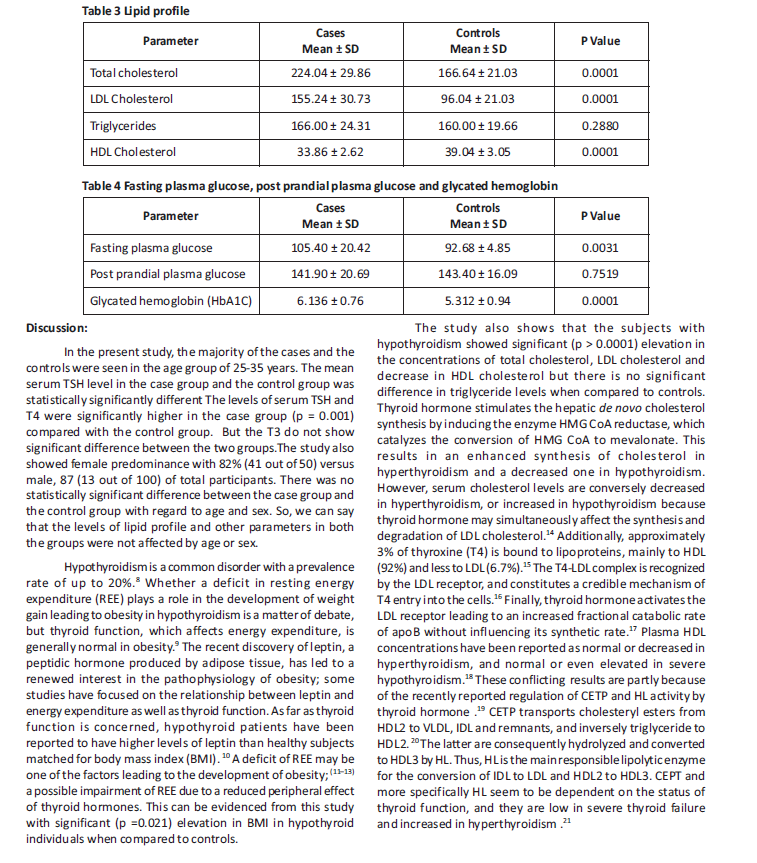
Thyroid hormones up regulate the expression of genes for GLUT-4 and phosphoglycerate kinase, involved in glucose transport and glycolysis respectively, thus acting synergistically with insulin in facilitating glucose disposal and utilization in peripheral tissue.22 In hypothyroidism because of altered metabolism of lipid and insulin, binding of insulin to insulin receptor decreases.23 Impaired translocation of GLUT-4 glucose transporters on plasma membrane occurs, resulting in decreased glucose uptake in muscles and adipose tissue occurs. But the results from our study showed only significant (0.003) elevation in fasting blood glucose in cases when compared to controls while the post prandial blood glucose do not significant (0.75) difference between the two groups. Even the fasting plasma glucose though elevated when compared to controls the mean value (105) has just crossed the upper normal limit. This indicates an impaired state with a chance of development of diabetes in future as the value is significantly high compared to controls.
The American Diabetes Association (ADA) have approved the use of HbA1c for the screening and the diagnosis of diabetes.24 The HbA1c concentration not only depends on prevailing glycaemia but also the life span of the erythrocytes and so, the conditions which affect the erythrocyte turnover or survival may lead to falsely elevate or lower the HbA1C levels.25 Recent studies have shown its spurious elevation in hypothyroidism in the absence of diabetes.26 Hypothyroidism is mainly complicated by normocytic normochromic anaemia which may be early iron deficiency anaemia due to nutritional deficiency or it may be secondary to hypothyroidism itself.27 The aetiology of anaemia in hypothyroidism can be related to the nutritional iron deficiency or to the endocrine disorder itself where the lowered thyroid hormone levels represses the bone marrow often resulting in decreased erythrocyte production which may affect the life span of erythrocytes. Altered erythrocyte life span may be partially responsible for spurious elevation in HbA1C levels.28-30 The value of HbA1c in the present study showed significant (0.0001) elevation in the cases when compared to controls but the value (6.1) does not cross the cutoff value of diagnosing diabetes. Even the value is not corresponding to the blood glucose values. It is inconclusive from this study whether to attribute the elevated HbA1c to impending diabetes or it is a spurious elevation as hemoglobin values were not evaluated to compare. Instead of HbA1c, we might have taken insulin levels which would be a more reliable parameter to assess glucose status. In Kuwaiti a study done by Al-Sayed A et al, on women to investigate the correlation between Subclinical hypothyroidism and insulin resistance, they found that the insulin levels were significantly higher in the Subclinical hypothyroidism group comparable to the normal control.31
Long-standing hypothyroidism is associated with several pathologic cardiovascular manifestations such as decreased intravascular volume, increased systemic vascular resistance, and hypertension.32 Most often, the alterations of cardiac performance are because of changes in the peripheral circulation. Hypertension is common in hypothyroidism and more specifically, diastolic hypertension may be present in approximately 20% of hypothyroid patients as seen in this study where there is a significant (0.0001) elevation in diastolic blood pressure in cases when compared to controls while there is no (0.73)significant difference in systolic blood pressure between the two groups..33 The coexistence of hypertension and lipid disorders in thyroid failure may accelerate the process of atherosclerosis. It is noteworthy that it has been demonstrated that thyroid hormone replacement therapy leads to a significant improvement of cardiovascular performance. 34 The decrease in blood pressure requires an optimum hormone replacement therapy and it might occur over a prolonged time course. 35
Conclusion
Thyroid hormone regulates the metabolism of lipids.
Thyroid disease may lead to lipid abnormalities that are associated with endothelium dysfunction, diastolic hypertension, and cardiovascular disease .Insulin resistance is a cardinal feature of type 2 diabetes mellitus and is relatively frequently found in mild thyroid dysfunction with increased risk of dyslipidemia. In recent times tremendous interest has been raised in the influence of thyroid hormone action on insulin levels. The development of insulin resistance leads to many metabolic abnormalities
Clinical significance
Thyroid dysfunction leads to altered glucose and lipid metabolism leading to insulin resistance, which is an important risk factor for cardio vascular diseases. Early detection of insulin resistance and prompt intervention for it in hypothyroid patients will be helpful to decrease cardiovascular morbidity and mortality. Only treatment of diabetes will not be that effective to resolve insulin resistance completely. Along with diabetes treatment, if we check and treat hypothyroidism even in subclinical stage then it will take care of its contribution to total insulin resistance.
REFERENCES
1. Annemike R, Stephen JL, Links Thera P, Gans Rijik OB Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. JCli Endo Metabolism. 2007; 92:491.
2. Bakker SJL, Ter Maten Jc, Pop sinjders C. The relationship between thyrotropin and low density lipoprotein cholesterol is modified by insulin sensitivity in healthy euthyroid subjects. Cli Endocrinol Metabolism. 2001; 86:1206-11. 59
3. Kutty KM, Bryant DG, Farid NR. Serum lipids in hypothyroidism-a re-evaluation. J Clin Endocrinol Metab 1978 Jan; 46(1):55-6.
4. Alireza Rastgooye Haghi et al Correlation Between Subclinical Hypothyroidism and Dyslipidemia Iranian journal of pathology. Vol.12 No.2 Spring 2017
5. Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39-51.
6. Peeyush Yadav, G.G.Kaushik, Sonali Sharma. Importance of Screening Type-II Diabetics for Thyroid Dysfunction and Dyslipidemia International Journal of Biochemistry and Biophysics 2015; 3(2): 7-12
7. Coller FA, Huggins CB. effect of hyperthyroidism upon diabetes mellitus: striking improvement in diabetes mellitus from thyroidectomy. Ann Surg. 1927 Dec;86(6):877-84.
8. Sawin CT, Castelli WP, Hershman JM, McNamara P,Bacharach P 1985 The aging thyroid: Thyroid deficiency in the Framingham study. Arch Intern Med 145:1386– 1388.
9. Goran MI. Energy metabolism and obesity. Med Clin North Am. 2000;84:347– 62.
10. Leonhardt U, Ritzel U, Schafer G, Becker W, Ramadori G. Serum leptin levels in hypo- and hyperthyroidism. J Endocrinol. 1998;157:75–9.
11. Carpenter WH, Fonong T, Toth MJ, et al. Total daily energy expenditure in free-living older African-Americans and Caucasians. Am J Physiol. 1998;274:E96 –101.
12. Foster GD, Wadden TA, Vogt RA. Resting energy expenditure in obese African American and Caucasian women.Obes Res. 1997;5:1– 8.
13. Wurmser H, Laessle R, Jacob K, et al. Resting metabolic rate in preadolescent girls at high risk of obesity. Int J Obes Relat Metab Disord. 1998;22:793–9.
14. Friis T, Pedersen LR 1987 Serum lipids in hyper- and hypothyroidism before and after treatment. Clin Chim Acta 162:155–163.
15. Benvenga S, Gregg R, Robbins J 1988 Binding of thyroxine hormone to human plasma lipoprotein. J Clin Endocrinol Metab 67:6–16.
16. Benvenga S, Robbins J 1990. Enhancement of thyroxine entry into low density lipoprotein (LDL) receptorcompetent fibroblasts by LDL: An additional mode of entry of thyroxine into cells. Endocrinology 126:933–941.
17. Statels B, van Tol A, Chan L, Will H, Verhoeven G, Auwerz J 1990 Alterations in thyroid status modulate apolipoprotein, hepatic triglyceride lipase and low density lipoprotein receptor in rats. Endocrinology 127:1144– 1152.
18. Scottolini AG, Bhagavan NV, Oshiro TH, Abe SY 1980 Serum high-density lipoprotein cholesterol concentrations in hypoand hyperthyroidism. Clin Chem 26:584–587.
19. Tan KCB, Shiu SWM, Kung AWC 1998 Plasma cholesteryl ester transfer protein activity in hyper- and hypothyroidism. J Clin Endocrinol Metab 83:149–153.
20. Lagrost L 1994 Regulation of cholesteryl ester transfer protein (CETP) activity: Review of in vitro and in vivo studies. Biochem Biophys Acta 1215:209–236.
21. Kussi T, Sacrinen P, Nikkila EA 1980 Evidence for the role of hepatic endothelial lipase in the metabolism of plasma high density lipoprotein2 in man. Atherosclerosis 36:589– 593.
22. Gould GW, Holmen GD. The glucose transporter family; structure,function and tissue specific expression Biochem journal. 1993;295-329.
23. Turner RC, Holman RR, Matthews D, Hockaday TD, Peto J. Insulin deficiency and insulin resistance interaction in diabetes: estimation of their relative contribution by feedback analysis from basal plasma insulin and glucose concentrations. Metabolism. 1979;28:1086-96.
24. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2011;34(Suppl. 1):S62-69. .
25. Gram-Hansen P, Eriksen J, Mourits-Andersen T, Olesen L. Glycosylated Haemoglobin (HbA1c) in iron and vitamin B12 deficiency. J Int Med. 1990;227:133-6.
26. Vij V, Chitnis P, Gupta VK. Evalution of thyroid dysfunction among type 2 diabetic patients. Int J Pharm Bio Sci. 2012;2:150-5.
27. Hardikar PS, Joshi SM, Bhat DS, Raut DA, Katre PA, et al. Spuriously high prevalence of prediabetes diagnosed by HbA1c in young Indians partly explained by haematological factors and iron deficiency anemia. Diabetes Care. 2012;35(4):797-802.
28. Horton L, Coburn RJ, England JM, Himsworth RL. The hematology of hypothyroidism Q J Med 1976;45(177): 101-23.
29. Das KC, Mukherjee M, Sarkar TK, Dash RJ, Rastogi GK. Erythropoiesis and erythropoietin in hypoand hyperthyroidism. J Clin Endocrinol Metab. 1975;40:211- 20.
30. Fein HG, Rivlin RS. Anaemia in thyroid diseases. Med Clin North Am. 1975;59:1133-45.
31. Al Sayed A, Al Ali N, Bo Abbas Y, Alfadhli E. Subclinical hypothyroidism is associated with early insulin resistance in Kuwaiti women. Endocr J. 2006;53(5):653-7.
32. Franklyn JA, Daykin J, Betteridge J, Hughes EA, Holder R, Jones SR, Sheppard MC 1993 Thyroxine replacement therapy and circulating lipid concentrations. Clin Endocrinol 38:453–459.
33. Klein I 1990 Thyroid hormone and the cardiovascular system. Am J Med 88:626–630.
34. Klein I, Ojamaa K 1992 Cardiovascular manifestations of endocrine disease. J Clin Endocrinol Metab 75:339–342. 35. Klemperer JD, Ojamaa K, Klein I 1996 Thyroid hormone therapy in cardiovascular disease. Prog Cardiovasc Dis 4:329–336.
How to cite this article : Usha kiran P, Sandeesha V, Lakshmana kumar N. Role of hypothyroidism in dyslipidemia and blood glucose regulation. Perspectives in Medical Research 2019; 7(2):56-61
Sources of Support: Nil,Conflict of interest:None declared
Year : 2019 | Volume : 7 | Issue : 2 Page : 56-61
Usha kiran P1, Sandeesha V2, Lakshmana kumar N,3
1Associate Professor, 2Assistant Professor, 3Professor and Head of the Department
Department(s) and institution(s)
Department of Biochemistry, GSL Medical college and General hospital
*Corresponding author: Dr.V.Sandeesha VAddress : Door No- 75-6-34, RK Hospital, Prakashnagar, Near Anand sweets Rajahmundry, Andhra Pradesh-533103
Phone numbers – 09491959817
Email ID: - [email protected]
Context:
Overt hypothyroidism is an established risk factor for insulin resistance and hyperlipidemia Aims: To evaluate the role of thyroid dysfunction on alteration of glucose and lipid metabolism leading to insulin resistance, an important risk factor for cardio vascular diseases. Setting and Design: In this study we included 50 subjects, aged 25 to 35 years. This is a case control study conducted in department of Biochemistry. Materials & Methods: Investigations like fasting and post prandial blood sugar, HbA1c and lipid profile (Cholesterol, Triglycerides, HDL, LDL & VLDL) were done. Blood pressure was measured. Body weight and height were measured and BMI was calculated. All the parameters were analyzed using XL 640 fully automated random access analyzer. Statistical analysis used: tudent t test was used using graph pad quickcalcs software.
Results:
The cases were selected based on T4 and TSH concentrations whose values were significantly decreased and elevated respectively. The patients with hypothyroidism exhibited significant increase in concentration of total cholesterol, LDL, fasting blood glucose and HbA1c while HDL (p<0.05) showed a decrease in its concentration in comparison to controls. BMI and diastolic blood pressure showed significant elevation in hypothyroid individuals when compared to controls.
Conclusions:
It is evident from this study that insulin resistance bears an indispensable role in connecting T2DM and thyroid dysfunction. Cardiovascular events are the counter reflection of resurgence of heavily disturbed lipid metabolism due to thyroid dyscrasias.
Keywords: Hypothyroidism, lipid profile, glycated hemoglobin, blood pressure and BMI
Key Messages:
Careful screening of patients with hypothyroidism is necessary to determine the lipid and diabetic status with the aim of timely treatment and prevention of the development of atherosclerosis and potential complications of atherosclerosis.
INTRODUCTION
Hypothyroidism is defined as a deficiency of thyroid activity. It results from reduced secretion of total thyroxine (T4) and triiodothyronin (T3). Hypothyroidism is a clinical syndrome due to deficiency of thyroid hormones which results in a generalized slowing down of metabolic process.1. Overt hypothyroidism is an established risk factor for insulin resistance and hyperlipidemia.2 Hyperlipidemia is one of the components of metabolic syndrome. In some studies, metabolic syndrome and its components (dyslipidemia) are responsible for 25%of the new onset cardiovascular disease (CVD).3 Thyroid hormones have an important regulatory effect on glucose and lipid metabolism, and blood pressure control.4
In iodine-replete areas, most persons with thyroid disorders have autoimmune disease, ranging from primary atrophic hypothyroidism, Hashimoto’s thyroiditis to thyrotoxicosis caused by Graves’ disease.5 Thyroid hormone action has long been recognized as an important determinant of glucose homeostasis.6 The role of hyperthyroidism in diabetes was investigated in 1927, by Coller and Huggins proving the association of hyperthyroidism and worsening of diabetes. It was shown that surgical removal of parts of thyroid gland had an ameliorative effect on the restoration of glucose tolerance in hyperthyroid patients suffering from coexisting diabetes.7
There is recent trend in cardiovascular sciences towards assessment of thyroid function in cardiac conditions as there is relation in between thyroid function and lipid metabolism which is risk factor for cardiac disease.we try to confirm this relationship with biochemical assays.
Thyroid hormones up regulate the expression of genes for GLUT-4 and phosphoglycerate kinase, involved in glucose transport and glycolysis respectively, thus acting synergistically with insulin in facilitating glucose disposal and utilization in peripheral tissue.22 In hypothyroidism because of altered metabolism of lipid and insulin, binding of insulin to insulin receptor decreases.23 Impaired translocation of GLUT-4 glucose transporters on plasma membrane occurs, resulting in decreased glucose uptake in muscles and adipose tissue occurs. But the results from our study showed only significant (0.003) elevation in fasting blood glucose in cases when compared to controls while the post prandial blood glucose do not significant (0.75) difference between the two groups. Even the fasting plasma glucose though elevated when compared to controls the mean value (105) has just crossed the upper normal limit. This indicates an impaired state with a chance of development of diabetes in future as the value is significantly high compared to controls.
The American Diabetes Association (ADA) have approved the use of HbA1c for the screening and the diagnosis of diabetes.24 The HbA1c concentration not only depends on prevailing glycaemia but also the life span of the erythrocytes and so, the conditions which affect the erythrocyte turnover or survival may lead to falsely elevate or lower the HbA1C levels.25 Recent studies have shown its spurious elevation in hypothyroidism in the absence of diabetes.26 Hypothyroidism is mainly complicated by normocytic normochromic anaemia which may be early iron deficiency anaemia due to nutritional deficiency or it may be secondary to hypothyroidism itself.27 The aetiology of anaemia in hypothyroidism can be related to the nutritional iron deficiency or to the endocrine disorder itself where the lowered thyroid hormone levels represses the bone marrow often resulting in decreased erythrocyte production which may affect the life span of erythrocytes. Altered erythrocyte life span may be partially responsible for spurious elevation in HbA1C levels.28-30 The value of HbA1c in the present study showed significant (0.0001) elevation in the cases when compared to controls but the value (6.1) does not cross the cutoff value of diagnosing diabetes. Even the value is not corresponding to the blood glucose values. It is inconclusive from this study whether to attribute the elevated HbA1c to impending diabetes or it is a spurious elevation as hemoglobin values were not evaluated to compare. Instead of HbA1c, we might have taken insulin levels which would be a more reliable parameter to assess glucose status. In Kuwaiti a study done by Al-Sayed A et al, on women to investigate the correlation between Subclinical hypothyroidism and insulin resistance, they found that the insulin levels were significantly higher in the Subclinical hypothyroidism group comparable to the normal control.31
Long-standing hypothyroidism is associated with several pathologic cardiovascular manifestations such as decreased intravascular volume, increased systemic vascular resistance, and hypertension.32 Most often, the alterations of cardiac performance are because of changes in the peripheral circulation. Hypertension is common in hypothyroidism and more specifically, diastolic hypertension may be present in approximately 20% of hypothyroid patients as seen in this study where there is a significant (0.0001) elevation in diastolic blood pressure in cases when compared to controls while there is no (0.73)significant difference in systolic blood pressure between the two groups..33 The coexistence of hypertension and lipid disorders in thyroid failure may accelerate the process of atherosclerosis. It is noteworthy that it has been demonstrated that thyroid hormone replacement therapy leads to a significant improvement of cardiovascular performance. 34 The decrease in blood pressure requires an optimum hormone replacement therapy and it might occur over a prolonged time course. 35
Conclusion
Thyroid hormone regulates the metabolism of lipids.
Thyroid disease may lead to lipid abnormalities that are associated with endothelium dysfunction, diastolic hypertension, and cardiovascular disease .Insulin resistance is a cardinal feature of type 2 diabetes mellitus and is relatively frequently found in mild thyroid dysfunction with increased risk of dyslipidemia. In recent times tremendous interest has been raised in the influence of thyroid hormone action on insulin levels. The development of insulin resistance leads to many metabolic abnormalities
Clinical significance
Thyroid dysfunction leads to altered glucose and lipid metabolism leading to insulin resistance, which is an important risk factor for cardio vascular diseases. Early detection of insulin resistance and prompt intervention for it in hypothyroid patients will be helpful to decrease cardiovascular morbidity and mortality. Only treatment of diabetes will not be that effective to resolve insulin resistance completely. Along with diabetes treatment, if we check and treat hypothyroidism even in subclinical stage then it will take care of its contribution to total insulin resistance.
REFERENCES
1. Annemike R, Stephen JL, Links Thera P, Gans Rijik OB Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. JCli Endo Metabolism. 2007; 92:491.
2. Bakker SJL, Ter Maten Jc, Pop sinjders C. The relationship between thyrotropin and low density lipoprotein cholesterol is modified by insulin sensitivity in healthy euthyroid subjects. Cli Endocrinol Metabolism. 2001; 86:1206-11. 59
3. Kutty KM, Bryant DG, Farid NR. Serum lipids in hypothyroidism-a re-evaluation. J Clin Endocrinol Metab 1978 Jan; 46(1):55-6.
4. Alireza Rastgooye Haghi et al Correlation Between Subclinical Hypothyroidism and Dyslipidemia Iranian journal of pathology. Vol.12 No.2 Spring 2017
5. Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39-51.
6. Peeyush Yadav, G.G.Kaushik, Sonali Sharma. Importance of Screening Type-II Diabetics for Thyroid Dysfunction and Dyslipidemia International Journal of Biochemistry and Biophysics 2015; 3(2): 7-12
7. Coller FA, Huggins CB. effect of hyperthyroidism upon diabetes mellitus: striking improvement in diabetes mellitus from thyroidectomy. Ann Surg. 1927 Dec;86(6):877-84.
8. Sawin CT, Castelli WP, Hershman JM, McNamara P,Bacharach P 1985 The aging thyroid: Thyroid deficiency in the Framingham study. Arch Intern Med 145:1386– 1388.
9. Goran MI. Energy metabolism and obesity. Med Clin North Am. 2000;84:347– 62.
10. Leonhardt U, Ritzel U, Schafer G, Becker W, Ramadori G. Serum leptin levels in hypo- and hyperthyroidism. J Endocrinol. 1998;157:75–9.
11. Carpenter WH, Fonong T, Toth MJ, et al. Total daily energy expenditure in free-living older African-Americans and Caucasians. Am J Physiol. 1998;274:E96 –101.
12. Foster GD, Wadden TA, Vogt RA. Resting energy expenditure in obese African American and Caucasian women.Obes Res. 1997;5:1– 8.
13. Wurmser H, Laessle R, Jacob K, et al. Resting metabolic rate in preadolescent girls at high risk of obesity. Int J Obes Relat Metab Disord. 1998;22:793–9.
14. Friis T, Pedersen LR 1987 Serum lipids in hyper- and hypothyroidism before and after treatment. Clin Chim Acta 162:155–163.
15. Benvenga S, Gregg R, Robbins J 1988 Binding of thyroxine hormone to human plasma lipoprotein. J Clin Endocrinol Metab 67:6–16.
16. Benvenga S, Robbins J 1990. Enhancement of thyroxine entry into low density lipoprotein (LDL) receptorcompetent fibroblasts by LDL: An additional mode of entry of thyroxine into cells. Endocrinology 126:933–941.
17. Statels B, van Tol A, Chan L, Will H, Verhoeven G, Auwerz J 1990 Alterations in thyroid status modulate apolipoprotein, hepatic triglyceride lipase and low density lipoprotein receptor in rats. Endocrinology 127:1144– 1152.
18. Scottolini AG, Bhagavan NV, Oshiro TH, Abe SY 1980 Serum high-density lipoprotein cholesterol concentrations in hypoand hyperthyroidism. Clin Chem 26:584–587.
19. Tan KCB, Shiu SWM, Kung AWC 1998 Plasma cholesteryl ester transfer protein activity in hyper- and hypothyroidism. J Clin Endocrinol Metab 83:149–153.
20. Lagrost L 1994 Regulation of cholesteryl ester transfer protein (CETP) activity: Review of in vitro and in vivo studies. Biochem Biophys Acta 1215:209–236.
21. Kussi T, Sacrinen P, Nikkila EA 1980 Evidence for the role of hepatic endothelial lipase in the metabolism of plasma high density lipoprotein2 in man. Atherosclerosis 36:589– 593.
22. Gould GW, Holmen GD. The glucose transporter family; structure,function and tissue specific expression Biochem journal. 1993;295-329.
23. Turner RC, Holman RR, Matthews D, Hockaday TD, Peto J. Insulin deficiency and insulin resistance interaction in diabetes: estimation of their relative contribution by feedback analysis from basal plasma insulin and glucose concentrations. Metabolism. 1979;28:1086-96.
24. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2011;34(Suppl. 1):S62-69. .
25. Gram-Hansen P, Eriksen J, Mourits-Andersen T, Olesen L. Glycosylated Haemoglobin (HbA1c) in iron and vitamin B12 deficiency. J Int Med. 1990;227:133-6.
26. Vij V, Chitnis P, Gupta VK. Evalution of thyroid dysfunction among type 2 diabetic patients. Int J Pharm Bio Sci. 2012;2:150-5.
27. Hardikar PS, Joshi SM, Bhat DS, Raut DA, Katre PA, et al. Spuriously high prevalence of prediabetes diagnosed by HbA1c in young Indians partly explained by haematological factors and iron deficiency anemia. Diabetes Care. 2012;35(4):797-802.
28. Horton L, Coburn RJ, England JM, Himsworth RL. The hematology of hypothyroidism Q J Med 1976;45(177): 101-23.
29. Das KC, Mukherjee M, Sarkar TK, Dash RJ, Rastogi GK. Erythropoiesis and erythropoietin in hypoand hyperthyroidism. J Clin Endocrinol Metab. 1975;40:211- 20.
30. Fein HG, Rivlin RS. Anaemia in thyroid diseases. Med Clin North Am. 1975;59:1133-45.
31. Al Sayed A, Al Ali N, Bo Abbas Y, Alfadhli E. Subclinical hypothyroidism is associated with early insulin resistance in Kuwaiti women. Endocr J. 2006;53(5):653-7.
32. Franklyn JA, Daykin J, Betteridge J, Hughes EA, Holder R, Jones SR, Sheppard MC 1993 Thyroxine replacement therapy and circulating lipid concentrations. Clin Endocrinol 38:453–459.
33. Klein I 1990 Thyroid hormone and the cardiovascular system. Am J Med 88:626–630.
34. Klein I, Ojamaa K 1992 Cardiovascular manifestations of endocrine disease. J Clin Endocrinol Metab 75:339–342. 35. Klemperer JD, Ojamaa K, Klein I 1996 Thyroid hormone therapy in cardiovascular disease. Prog Cardiovasc Dis 4:329–336.
How to cite this article : Usha kiran P, Sandeesha V, Lakshmana kumar N. Role of hypothyroidism in dyslipidemia and blood glucose regulation. Perspectives in Medical Research 2019; 7(2):56-61
Sources of Support: Nil,Conflict of interest:None declared

Open Access
Perspectives in Medical Research is committed to keeping research articles Open Access.Journal permits any users to read, download, copy, print, search, or link to the full texts of these articles...
Read more
© PIMR.org.in - 2013. All Rights Reserved.