
advertise here
Original Articles
EVALUATION OFTRANSVERSUSABDOMINIS PLANE (TAP) BLOCK WITH
INJ.BUPIVACAINE 0.25% FOR POST-OPERATIVE ANALGESIA IN INGUINAL HERNIA
REPAIR SURGERY.
Year : 2019 | Volume : 7 | Issue : 3 Page : 30-37
Abstract
Background:
TransversusAbdominis Plane(TAP)Block is a regional analgesictechnique. It provides postoperative analgesia after lower abdominal surgery. The purpose of our study was to evaluate effectiveness of TAP block to provide effective postoperative analgesia in patients undergoing inguinal hernia repair surgery.
Method:
Total 60 patients undergoing inguinal hernia surgery were randomized toundergo TAP block with bupivacaine (n = 30) versus normal saline (n = 30)control group. All patients received a standard spinal anaesthesia with standardmonitoring. A TAP block was performed using 20 ml 0.25% bupivacaine on the side ofsurgery or 20 ml saline at the end of surgery. Each patient was followed uppostoperatively at 0, 30 min, 60 min, 2 hr, 4, 6, 8, 12, 18 and 24 hours in PACU. Rescue analgesics inj. Diclofenacwere offered to any patient whocomplained of pain (VAS Score ≥4). Time of rescueanalgesia, total analgesic consumption and any other complications wereassessed.
Result :
There was a significantly longer time to the first request for rescue analgesic in bupivacaine group. (507.77 ± 10.38 min) compared to NS group.(110.87±14.2min) Total diclofenacconsumptionwas significantly higher in Group S than Group B (82.75 ± 23.2 mg vs193.97 ± 37.6 mg).
Conclusion :
TAP block provides better postoperative analgesia in patient undergoing inguinalhernia repair surgery . It prolongs the duration of postoperative analgesia and significantly reduces the total analgesic consumption up to 24 hrs postoperatively.
Keywords :
TAP block, Bupivacaine, postoperative analgesia.
Introduction
TransversusAbdominis Plane (TAP) block is a regional anaesthesia technique. It can be used as a technique to provide postoperative analgesia in surgeries involving lower abdomen like inguinal hernia surgery, abdominal hysterectomy, caesarean section etc. Usually an opioid or a NSAID is prescribed for postoperative analgesia. The opioids have side effects like, vomiting, reduced gut motility, sedation, respiratory depression etc.NSAIDS have certain side effects like renal dysfunction, gastritis,Gastrointestinal bleeding, etc. but TAP block has minimal systemic side effects thus sparing the Use of opioids and NSAIDS which can result in significant adverse effects.
TAP block was first introduced by Rafi et al in 20011 as a landmark technique and was further developed and tested by McDonnell et al in 2004 2. . It is giventhrough the lumbar triangle of petit which is formed by external oblique muscle anteriorly, lattismusdorsi muscle posteriorly, iliac crest inferiorly and is identified as a defect 1 cm above the iliac crest in mid axillary line. It involves injection of a local anaesthetic solution in to a plane between the internal oblique and transversusabdominis muscle. Since the thoracolumbar nerves originating from the T6-L1 spinal roots run in to the plane and supply the sensory nerves to the anterior abdominal wall the local anaesthetic spread in this plane can blocks these nerves and provide analgesia to the anterior abdominal wall
The purpose of our study was to evaluate effectiveness of TAP block toprovide effective postoperative analgesia in patients undergoing inguinal herniarepair surgery.
Material and Method
After Ethical Committee approval, we conducted the study on sixty male patientsundergoing unilateral inguinal hernioplasty. Our study was conducted in a tertiary care hospital. The study was a randomized, double-blinded, controlled clinical study. Patient were divided into 2 groups of 30 each. Randomization of the patients was done using computerized randomization charts in to two groups by computer generated tables to undergo TAP block with bupivacaine 0.25% 20 ml (n =30) [GROUP B] which is the Study group versus normal saline 20 ml (n=30) [GROUP S], the control group. Blinding was maintained as the person injecting the solution while giving TAPblock was unaware of whether it is normal saline or bupivacaine as it was preparedby another person in operation theatre. Pre anesthetic check-up was done.
Inclusion criteria were male patients giving written and informed consent for the study, ASA grade I & II, age group 20 to 65 yrsundergoing unilateral inguinal hernia surgery under spinal anaesthesia. Exclusion criteria were Patient refusal, bleeding disorders, allergy to local anaesthetics, mental disorders, morbid obesity, abnormal liver function tests, infection at local site of block. Thorough pre anaesthetic evaluation with routine investigations like complete blood count, urine routine, liver and renal function tests, bleeding time / clotting time, random blood sugar, Chest x ray, ECG and Serum electrolytes were done.
Consent and fasting status was confirmed. In the operation theatre, standardmonitoring including ECG, noninvasive BP, pulse oximeter were attached. Peripheralline was taken with 18G IV cannula. All patients receivedstandardized spinal anaesthesia with 0.5% bupivacaine 3.5 ml in sitting position. Levelof analgesia achieved noted. No analgesic or sedation was given to patient. Intraoperatively vitals were monitored. The TAP block was performed at the end of the surgery following all asepticprecautions using the following technique. A 22-gauge 1 ½” blunt tipped hypodermicneedle attached with flexible tubing to a syringe filled with the study solution wasused. With the patient in a supine position the triangle of Petit was palpated between the anterior border of latissimusdorsi, the posterior border of the external oblique, and the iliac crest.
Needle was introduced perpendicularly through the triangle and advanced until two “ POPS” or “ give ways” were felt. After careful aspiration the drug was deposited in the fascial plane. Patient was further observed for 15 minutes and shifted to post anaesthesiacare unit. Patient monitored at 30 min, 60 min,2, 4, 6 ,12 ,18, 24 hrs post operatively forpulse rate, BP, RR, pain by VAS score and complications if any. Pain was assessed by visual analogue score from 0 to 10. Patient was given rescue analgesia in the form of intramuscular Diclofenac 75 mg at VAS score of 4. Patient monitored for the time to first analgesic usage and also the total no. of analgesic doses required in first 24hrs. The duration of analgesia in TAPB was considered the first request for postoperative analgesia after surgery. Patient was also observed for any other postoperative complications.
Statistical evaluation was done by applying Chi-Square statistics. Data was collected tabulated and then analysed.data was expressed as mean and standard deviation, median and ranges. Statistical analysis was performed with SPSS version 15.
Result
In this randomized, double-blind, controlled comparative clinical study, we studied 60 ASA physical status I & II patients scheduled for Unilateral inguinal hernioplasty in our hospital, in the time period between December 2015 to June 2017.All 60 patients undergoing inguinal hernioplasty were randomized to undergo TAP block with 0.25% bupivacaine (n = 30) [Group B] versus normal saline (n= 30) [Group S]. They all received a standard spinal anaesthesia with standard monitoring, TAP block was performed using 0.25% bupivacaine 20 ml or 20 ml saline on the side of surgery at the end of surgery after skin closure. Same investigator performed TAP block in all the patients.
In our randomized controlled trial, TAP block with normal saline was given topatients who were included in control group for blinding purpose and we aimed toevaluate the efficacy of transversusabdominis plane block.
Demographic profile
Table No. 1 Demographic data
Majority of the patient were in age group of 30 to 50 in both group. Both groups were comparable in terms of age, weight and height. No significant difference was observed between two groups in terms of demographic data.
Comparison of vas score:
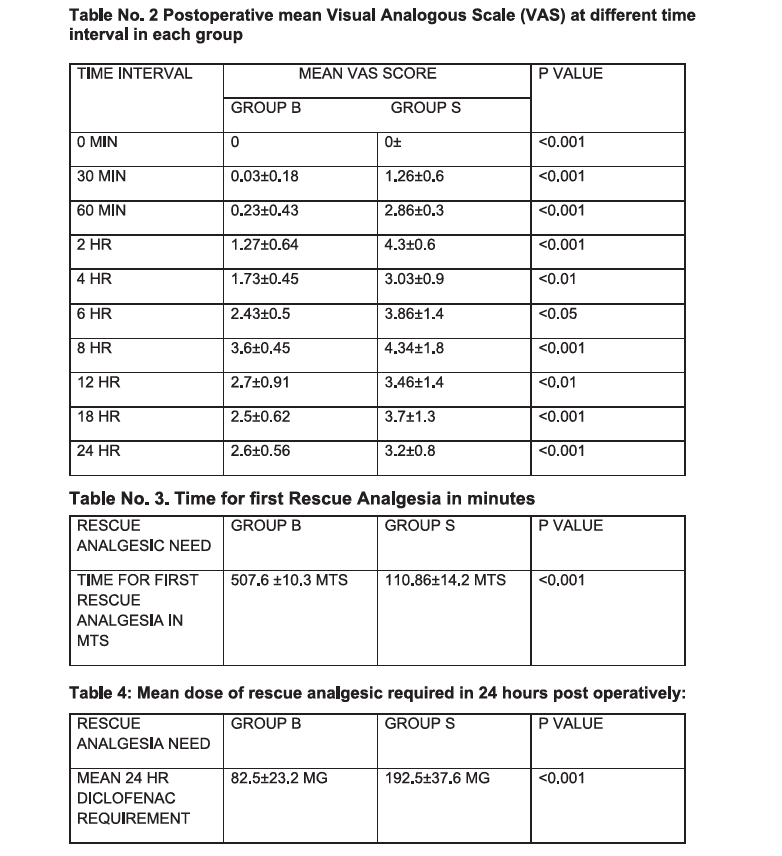
Table No. 2 Postoperative mean Visual Analogous Scale (VAS) at different timeinterval in each group VAS score was significantly higher in control group as compared to the study group at all the time in first 24 hours.
Postoperative Rescue Analgesic requirement
Table No. 3. Time for first Rescue Analgesia in minutes
First dose of rescue analgesia required in study group was at 507.6± 10.3 min and in control group was 110.86 ± 14.2 min which was statistically significant.
Table 4: Mean dose of rescue analgesic required in 24 hours post operatively:
Total dose of Diclofenac consumption in study group was 82.5±23.2mg and in control group it was 192.5±37.6mg, which showed that Diclofenac consumption was significantly decreased in study group.
Table 5: No of diclofenac injections consumed in 24 hrs Diclofenac requirement in study group was one time in 27 patient and two time in 3 patient which was significantly less as compare to control group in which diclofenac requirement was one time in 1 patient and two time in 14 patient and three time in 15 patient in 24 hour. There were no any complications related to the TAP block technique in both the groups.
Discussion
Elective inguinal hernia repair is one of the most common surgical procedures performed..Pain after inguinal hernia repair is more pronounced in the first two postoperative days. The pain is aggravated during mobilisation or coughing. Adequate postoperative analgesia facilitates earlier patient mobilization and earlier fulfilment of discharge criteria from postoperative wards.
Various methods and medications are used in postoperative pain management.The most common approach to post-operative pain relief is multimodal using NSAIDs,opioids and local infiltration of local anesthetic. Opioids and NSAIDS have their own side effects. Local infiltration does not relieve deep muscular pain Hence we thought of an alternative technique in the form of unilateral TAP block with 0.25% of Bupivacaine at the end of surgery to evaluate the efficacy of TAP block with requirement of other analgesic drugs.
In this study we decided to give TAP block by landmark technique after completion of surgery for postoperative analgesia as effect of spinal anaesthesia wear off in 2 to 3 hours.The results of our study showed that patients who received TAP block with local anaesthestic had 8 to 9hour duration of analgesia. This was similar to the study performed by Mc Donnell et al 2in caesarean section delivery where VAS at rest and on movement was significantly low till 12 hours in patients who received TAP block with local anaesthetic. Study performed by Niraj et al 3in open appendicectomy and NeerjaBharti et al4 in colorectal surgery also showed similar results. In accordance with the present study, Ila B. Patelet al5observed in their study that VAS score ≥ 4 was achieved in patients given TAP block with inj. Bupivacaine 0.25% at 10-11 hours while in control group it was at 2-3 hours.NehaFuladi et al 6and Neha Sharma et al7in their study observed that VAS score ≥4 was achieved in patients given TAP block with inj. Bupivacaine 0.25% at 12 hours while in control group it was at 6 hours. DilekErdoğan Arı et al8observed that VAS score ≥4 was achieved in patient given TAP block with inj. Bupivacaine 0.25% at 3 hours postoperatively which was far lesscompared to our study.
Total dose of diclofenac consumption in group B was 82.75±23.2 mg and ingroup S it was 193.97±37.6 mg which showed that diclofenac consumption was significantly decreased in group S .One important measure of analgesic efficacy in our study was requirement ofdiclofenac during first 24hrs. The 24hrs consumption of total diclofenac was 57%less in Group B as compared to Group S. The results of our study are similar to the study done by Ila B. Patelet al 5theyobserved that Total dose of diclofenac consumption in TAP block group with inj.Bupivacaine 0.25% was 95 ± 33.73 mg and control group it was 202.5 ± 44.69mg.TauqeerAnjum Mir et al9, Muhammad TahseenTalib et al10, Dr.Dipika Patel et al11 , Niraj et al3, John Carney et al12 also found decreased analgesic requirements postoperatively within 24 hour which was similar to our study.
Complication that can occur with TAP block include bowel puncture, nerve injury and puncture of the liver. Faroog M, Carey M13reported a case of liver trauma with blunt regionalanaesthesia needle while performing TAP block. We did not observe any of these complications by landmark technique.
Conclusion
TAP block is a promising technique in alleviating postoperative pain in patients undergoing lower abdominal surgeries. Simplicity of this block, along with reliable level of analgesia, longer duration as well as good quality with lesser rescue analgesics requirement and their side-effects makes the TAP block a good option for postoperative analgesia in lower abdominal surgeries.
REFERENCES:
1- Rafi A. Abdominal field block: a new approach via the lumbar triangle.Anaesthesia 2001; 56: 1024-26.
2- McDonnell J, O' Donnell B, Tuite D, Farrell T, Power C. The regional abdominal field infiltration (R.A.F.I.) technique: computerized tomographic and anatomicalidentification of a novel approach to the transverses abdominisneuro-vascular fascialplane. Anaesthesiology 2004; 101: A 899
3- G. Niraj, A. Searle, M. Mathews, V. Misra, M. Baban, S. Kiani, M. Wong BJA: Analgesicefficacy of ultrasound-guided transversusabdominis plane block in patients undergoingopen appendicectomy, Br. J. Anaesth. (2009) 103 (4): 601-605.
4- NeerjaBharti, Parag Kumar, InduBala, Vikas Gupta, The Efficacy of a NovelApproach to TransversusAbdominis Plane Block for Postoperative Analgesia AfterColorectal Surgery, Anaesthesia Analgesia2011;112:1504–8
5- Ila B. Patel, Alka P. Shah and Anil Kumar Bhiwal 2015. Evaluation of TransversusAbdominis Plane (TAP) Block in Abdominal Surgery by Total Requirement of Diclofenac asa PostOperative Analgesia drug.Ila B. Patel et al/ International Journal of BiomedicalResearch 2015; 6(10): 841-846.


Year : 2019 | Volume : 7 | Issue : 3 Page : 30-37
Nandanwankar N K1,Abdullah M F2
1. Associate professor ,Department of Anaesthesiology, Dr.ShankarraoChavanGovt Medical college, Nanded (Maharashtra)
2. ICU Registrar ,Dr.Rela Institute and Medical centre, Chennai
Address for correspondence Dr.SUBHARANJAN SAMANTARAY. C-Blook 303 Prathima institute of medical sciences, Karimnagar
Mob no:7972165107
E-mail:[email protected]
Abstract
Background:
TransversusAbdominis Plane(TAP)Block is a regional analgesictechnique. It provides postoperative analgesia after lower abdominal surgery. The purpose of our study was to evaluate effectiveness of TAP block to provide effective postoperative analgesia in patients undergoing inguinal hernia repair surgery.
Method:
Total 60 patients undergoing inguinal hernia surgery were randomized toundergo TAP block with bupivacaine (n = 30) versus normal saline (n = 30)control group. All patients received a standard spinal anaesthesia with standardmonitoring. A TAP block was performed using 20 ml 0.25% bupivacaine on the side ofsurgery or 20 ml saline at the end of surgery. Each patient was followed uppostoperatively at 0, 30 min, 60 min, 2 hr, 4, 6, 8, 12, 18 and 24 hours in PACU. Rescue analgesics inj. Diclofenacwere offered to any patient whocomplained of pain (VAS Score ≥4). Time of rescueanalgesia, total analgesic consumption and any other complications wereassessed.
Result :
There was a significantly longer time to the first request for rescue analgesic in bupivacaine group. (507.77 ± 10.38 min) compared to NS group.(110.87±14.2min) Total diclofenacconsumptionwas significantly higher in Group S than Group B (82.75 ± 23.2 mg vs193.97 ± 37.6 mg).
Conclusion :
TAP block provides better postoperative analgesia in patient undergoing inguinalhernia repair surgery . It prolongs the duration of postoperative analgesia and significantly reduces the total analgesic consumption up to 24 hrs postoperatively.
Keywords :
TAP block, Bupivacaine, postoperative analgesia.
Introduction
TransversusAbdominis Plane (TAP) block is a regional anaesthesia technique. It can be used as a technique to provide postoperative analgesia in surgeries involving lower abdomen like inguinal hernia surgery, abdominal hysterectomy, caesarean section etc. Usually an opioid or a NSAID is prescribed for postoperative analgesia. The opioids have side effects like, vomiting, reduced gut motility, sedation, respiratory depression etc.NSAIDS have certain side effects like renal dysfunction, gastritis,Gastrointestinal bleeding, etc. but TAP block has minimal systemic side effects thus sparing the Use of opioids and NSAIDS which can result in significant adverse effects.
TAP block was first introduced by Rafi et al in 20011 as a landmark technique and was further developed and tested by McDonnell et al in 2004 2. . It is giventhrough the lumbar triangle of petit which is formed by external oblique muscle anteriorly, lattismusdorsi muscle posteriorly, iliac crest inferiorly and is identified as a defect 1 cm above the iliac crest in mid axillary line. It involves injection of a local anaesthetic solution in to a plane between the internal oblique and transversusabdominis muscle. Since the thoracolumbar nerves originating from the T6-L1 spinal roots run in to the plane and supply the sensory nerves to the anterior abdominal wall the local anaesthetic spread in this plane can blocks these nerves and provide analgesia to the anterior abdominal wall
The purpose of our study was to evaluate effectiveness of TAP block toprovide effective postoperative analgesia in patients undergoing inguinal herniarepair surgery.
Material and Method
After Ethical Committee approval, we conducted the study on sixty male patientsundergoing unilateral inguinal hernioplasty. Our study was conducted in a tertiary care hospital. The study was a randomized, double-blinded, controlled clinical study. Patient were divided into 2 groups of 30 each. Randomization of the patients was done using computerized randomization charts in to two groups by computer generated tables to undergo TAP block with bupivacaine 0.25% 20 ml (n =30) [GROUP B] which is the Study group versus normal saline 20 ml (n=30) [GROUP S], the control group. Blinding was maintained as the person injecting the solution while giving TAPblock was unaware of whether it is normal saline or bupivacaine as it was preparedby another person in operation theatre. Pre anesthetic check-up was done.
Inclusion criteria were male patients giving written and informed consent for the study, ASA grade I & II, age group 20 to 65 yrsundergoing unilateral inguinal hernia surgery under spinal anaesthesia. Exclusion criteria were Patient refusal, bleeding disorders, allergy to local anaesthetics, mental disorders, morbid obesity, abnormal liver function tests, infection at local site of block. Thorough pre anaesthetic evaluation with routine investigations like complete blood count, urine routine, liver and renal function tests, bleeding time / clotting time, random blood sugar, Chest x ray, ECG and Serum electrolytes were done.
Consent and fasting status was confirmed. In the operation theatre, standardmonitoring including ECG, noninvasive BP, pulse oximeter were attached. Peripheralline was taken with 18G IV cannula. All patients receivedstandardized spinal anaesthesia with 0.5% bupivacaine 3.5 ml in sitting position. Levelof analgesia achieved noted. No analgesic or sedation was given to patient. Intraoperatively vitals were monitored. The TAP block was performed at the end of the surgery following all asepticprecautions using the following technique. A 22-gauge 1 ½” blunt tipped hypodermicneedle attached with flexible tubing to a syringe filled with the study solution wasused. With the patient in a supine position the triangle of Petit was palpated between the anterior border of latissimusdorsi, the posterior border of the external oblique, and the iliac crest.
Needle was introduced perpendicularly through the triangle and advanced until two “ POPS” or “ give ways” were felt. After careful aspiration the drug was deposited in the fascial plane. Patient was further observed for 15 minutes and shifted to post anaesthesiacare unit. Patient monitored at 30 min, 60 min,2, 4, 6 ,12 ,18, 24 hrs post operatively forpulse rate, BP, RR, pain by VAS score and complications if any. Pain was assessed by visual analogue score from 0 to 10. Patient was given rescue analgesia in the form of intramuscular Diclofenac 75 mg at VAS score of 4. Patient monitored for the time to first analgesic usage and also the total no. of analgesic doses required in first 24hrs. The duration of analgesia in TAPB was considered the first request for postoperative analgesia after surgery. Patient was also observed for any other postoperative complications.
Statistical evaluation was done by applying Chi-Square statistics. Data was collected tabulated and then analysed.data was expressed as mean and standard deviation, median and ranges. Statistical analysis was performed with SPSS version 15.
Result
In this randomized, double-blind, controlled comparative clinical study, we studied 60 ASA physical status I & II patients scheduled for Unilateral inguinal hernioplasty in our hospital, in the time period between December 2015 to June 2017.All 60 patients undergoing inguinal hernioplasty were randomized to undergo TAP block with 0.25% bupivacaine (n = 30) [Group B] versus normal saline (n= 30) [Group S]. They all received a standard spinal anaesthesia with standard monitoring, TAP block was performed using 0.25% bupivacaine 20 ml or 20 ml saline on the side of surgery at the end of surgery after skin closure. Same investigator performed TAP block in all the patients.
In our randomized controlled trial, TAP block with normal saline was given topatients who were included in control group for blinding purpose and we aimed toevaluate the efficacy of transversusabdominis plane block.
Demographic profile
Table No. 1 Demographic data
Majority of the patient were in age group of 30 to 50 in both group. Both groups were comparable in terms of age, weight and height. No significant difference was observed between two groups in terms of demographic data.
Comparison of vas score:
Table No. 2 Postoperative mean Visual Analogous Scale (VAS) at different timeinterval in each group VAS score was significantly higher in control group as compared to the study group at all the time in first 24 hours.
Postoperative Rescue Analgesic requirement
Table No. 3. Time for first Rescue Analgesia in minutes
First dose of rescue analgesia required in study group was at 507.6± 10.3 min and in control group was 110.86 ± 14.2 min which was statistically significant.
Table 4: Mean dose of rescue analgesic required in 24 hours post operatively:
Total dose of Diclofenac consumption in study group was 82.5±23.2mg and in control group it was 192.5±37.6mg, which showed that Diclofenac consumption was significantly decreased in study group.
Table 5: No of diclofenac injections consumed in 24 hrs Diclofenac requirement in study group was one time in 27 patient and two time in 3 patient which was significantly less as compare to control group in which diclofenac requirement was one time in 1 patient and two time in 14 patient and three time in 15 patient in 24 hour. There were no any complications related to the TAP block technique in both the groups.
Discussion
Elective inguinal hernia repair is one of the most common surgical procedures performed..Pain after inguinal hernia repair is more pronounced in the first two postoperative days. The pain is aggravated during mobilisation or coughing. Adequate postoperative analgesia facilitates earlier patient mobilization and earlier fulfilment of discharge criteria from postoperative wards.
Various methods and medications are used in postoperative pain management.The most common approach to post-operative pain relief is multimodal using NSAIDs,opioids and local infiltration of local anesthetic. Opioids and NSAIDS have their own side effects. Local infiltration does not relieve deep muscular pain Hence we thought of an alternative technique in the form of unilateral TAP block with 0.25% of Bupivacaine at the end of surgery to evaluate the efficacy of TAP block with requirement of other analgesic drugs.
In this study we decided to give TAP block by landmark technique after completion of surgery for postoperative analgesia as effect of spinal anaesthesia wear off in 2 to 3 hours.The results of our study showed that patients who received TAP block with local anaesthestic had 8 to 9hour duration of analgesia. This was similar to the study performed by Mc Donnell et al 2in caesarean section delivery where VAS at rest and on movement was significantly low till 12 hours in patients who received TAP block with local anaesthetic. Study performed by Niraj et al 3in open appendicectomy and NeerjaBharti et al4 in colorectal surgery also showed similar results. In accordance with the present study, Ila B. Patelet al5observed in their study that VAS score ≥ 4 was achieved in patients given TAP block with inj. Bupivacaine 0.25% at 10-11 hours while in control group it was at 2-3 hours.NehaFuladi et al 6and Neha Sharma et al7in their study observed that VAS score ≥4 was achieved in patients given TAP block with inj. Bupivacaine 0.25% at 12 hours while in control group it was at 6 hours. DilekErdoğan Arı et al8observed that VAS score ≥4 was achieved in patient given TAP block with inj. Bupivacaine 0.25% at 3 hours postoperatively which was far lesscompared to our study.
Total dose of diclofenac consumption in group B was 82.75±23.2 mg and ingroup S it was 193.97±37.6 mg which showed that diclofenac consumption was significantly decreased in group S .One important measure of analgesic efficacy in our study was requirement ofdiclofenac during first 24hrs. The 24hrs consumption of total diclofenac was 57%less in Group B as compared to Group S. The results of our study are similar to the study done by Ila B. Patelet al 5theyobserved that Total dose of diclofenac consumption in TAP block group with inj.Bupivacaine 0.25% was 95 ± 33.73 mg and control group it was 202.5 ± 44.69mg.TauqeerAnjum Mir et al9, Muhammad TahseenTalib et al10, Dr.Dipika Patel et al11 , Niraj et al3, John Carney et al12 also found decreased analgesic requirements postoperatively within 24 hour which was similar to our study.
Complication that can occur with TAP block include bowel puncture, nerve injury and puncture of the liver. Faroog M, Carey M13reported a case of liver trauma with blunt regionalanaesthesia needle while performing TAP block. We did not observe any of these complications by landmark technique.
Conclusion
TAP block is a promising technique in alleviating postoperative pain in patients undergoing lower abdominal surgeries. Simplicity of this block, along with reliable level of analgesia, longer duration as well as good quality with lesser rescue analgesics requirement and their side-effects makes the TAP block a good option for postoperative analgesia in lower abdominal surgeries.
REFERENCES:
1- Rafi A. Abdominal field block: a new approach via the lumbar triangle.Anaesthesia 2001; 56: 1024-26.
2- McDonnell J, O' Donnell B, Tuite D, Farrell T, Power C. The regional abdominal field infiltration (R.A.F.I.) technique: computerized tomographic and anatomicalidentification of a novel approach to the transverses abdominisneuro-vascular fascialplane. Anaesthesiology 2004; 101: A 899
3- G. Niraj, A. Searle, M. Mathews, V. Misra, M. Baban, S. Kiani, M. Wong BJA: Analgesicefficacy of ultrasound-guided transversusabdominis plane block in patients undergoingopen appendicectomy, Br. J. Anaesth. (2009) 103 (4): 601-605.
4- NeerjaBharti, Parag Kumar, InduBala, Vikas Gupta, The Efficacy of a NovelApproach to TransversusAbdominis Plane Block for Postoperative Analgesia AfterColorectal Surgery, Anaesthesia Analgesia2011;112:1504–8
5- Ila B. Patel, Alka P. Shah and Anil Kumar Bhiwal 2015. Evaluation of TransversusAbdominis Plane (TAP) Block in Abdominal Surgery by Total Requirement of Diclofenac asa PostOperative Analgesia drug.Ila B. Patel et al/ International Journal of BiomedicalResearch 2015; 6(10): 841-846.

Open Access
Perspectives in Medical Research is committed to keeping research articles Open Access.Journal permits any users to read, download, copy, print, search, or link to the full texts of these articles...
Read more
© PIMR.org.in - 2013. All Rights Reserved.