
advertise here
Original Article
A Study on surgical management of distal humerus fractures in adults by
open reduction and internal fixation
Year : 2019 | Volume : 7 | Issue : 2 Page : 26-30
Distal humerus fractures represent one of the most complicated and challenging fractures in the upper extremity. Distal humerus fractures in adults are difficult fractures to treat because of significant comminution and they are rare fractures which prevents the individual surgeon from accumulating sufficient personal experience to critically evaluate the results of the treatment.
Aims & Objectives:
1. To evaluate the role of operative management in distal humerus fractures. 2. To follow up & evaluate results on patients operated upon and note the functional outcome and complications.
Patients and Methods:
The present study is a prospective study of 30 cases of Distal humerus fractures (AO Type 13.A, 13.B and 13.C, 12 male and 18 females, age ranging from 20 to 70) treated by open reduction and internal fixation over two years, from September 2016 to August 2018 was conducted in department of orthopaedics, Prathima institute of medical sciences, Karimnagar. All patients were selected among admissions, operated and results were assessed clinically and radiographically. The functional evaluation of the results Cassebaum’s scale has been chosen. The follow up period ranges with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks and complications noted.
Results:
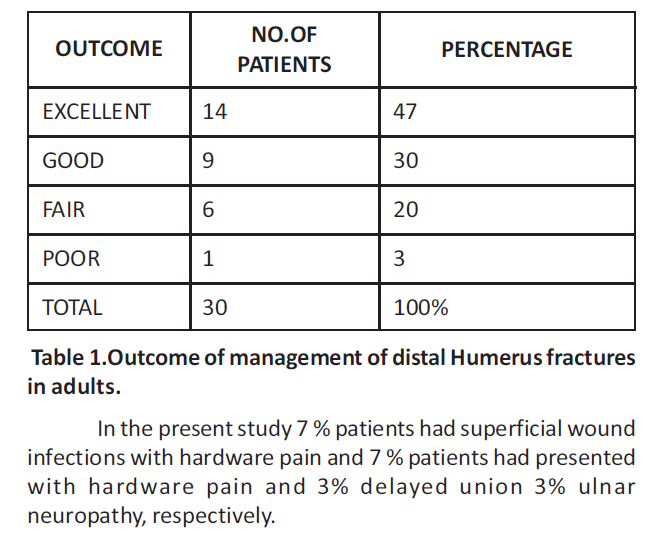
Outcome of surgical management of distal humerus fractures in adults by open reduction and interal fixation was evaluated using Cassebaum scale it was observed that 47% cases presented with excellent outcome, 30% cases presented with good outcome, 20% cases presented with fair outcome, 1% cases presented with poor outcome. In the present study 7% patients had superficial wound infections with hardware pain and 7% patients had presented with hardware pain and 3% delayed union 3% ulnar neuropathy, respectively.
Conclusion:
The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable, in restoring articular surface and early rehabilitation which decreases morbidity, resulting good functional outcome. Keywords:
distal humerus fracture, Cassebaum’s scale, open reduction and internal fixation, dual plates, AO: Arbeitsgemeinschaft Fur Osteosynthesefragen. INTRODUCTION
Distal humerus fractures represent one of the most complicated and challenging fractures in the upper extremity. Distal humerus fractures in adults are difficult fractures to treat because of significant comminution and they are rare fractures which prevents the individual surgeon from accumulating sufficient personal experience to critically evaluate the results of the treatment. The results of managing these fractures nonoperatively are limited by failure to get anatomical reduction and early mobilization, which often results in painful stiff elbow and/or pseudarthrosis. Hence an operative management with anatomical reduction of the fragments becomes the treatment of choice for these fractures1. The complex three-dimensional geometry of the distal humerus poses a considerable challenge to reconstruction2.
The distal humerus fractures are rare fractures constituting 2%3 of all body fractures. Watson and Jones4 wrote “few fractures are more difficult to treat” while describing them, thus describing their complexity. The forearm musculature originating on the condyles tends to produce rotational displacement even when closed reduction is achieved. The only reliable method for restoring the normal alignment and contour of the distal humerus is operative exposure and direct manipulation of fracture fragments. However, fixation of fracture fragments must be stable enough to allow motion while ensuring union. In most cases open reduction with stable rigid internal fixation is required to fulfil the above goal.
The recommendations for treatment have ranged widely from essentially no treatment to operative reduction and extensive internal fixation. In some of these fractures particularly those with intra articular comminution, anatomical restoration of the articular surface cannot be adequately achieved or maintained through manipulative reduction alone.
Critics of open reduction have argued that the additional surgical trauma and the inherent difficulty in securely stabilizing the small intra articular fragments will lead to added fibrosis and a less satisfactory result. Even those who have recommended operative treatment differ widely in their opinions with regard to extent, approach, type of internal fixation to be used and when to start the post-operative mobilization.
The recent trend has been immediate open reduction, stable and rigid internal fixation and early post-operative mobilization. The anatomic complexity of distal humerus makes surgical reconstruction difficult. The fabrication of newer implants however, has increased the reliability of the operative stabilization, while placing additional demands on the surgeon expertise.
Injuries of the elbow lead to chronic pain and permanent restriction of motion, limiting the use of hand in basic daily activities from eating to personal hygiene require a wide range of positions and movements at the elbow in flexion, extension and forearm rotation. Recent advances in surgical techniques and equipment designed to make possible rigid osteosynthesis of smaller intra articular fragments which permits early post-operative rehabilitation and achieve improved results.
Patients and Methods:
A prospective study to evaluate the role of open reduction and internal fixation in the treatment of distal humerus fractures. Patients selected for this operation were of different ages and genders, admitted and treated in Prathima Institute of Medical Sciences, Karimnagar during the years 2016-2018. The classification criteria used was AO classification in which most of them were AO type 13.A and remaining were AO type 13.B and AO type 13.C
A thorough general examination and local examination was performed. Radiological examination of the part and routine investigations were carried out. Patients were taken up for surgery as early as possible in all the cases. Old people with medical problems after thorough work up were taken up once the patient is fit for surgery. Pre operatively all patients were immobilized in above elbow plaster of paris slab with elevation of limb. Associated injuries were dealt simultaneously or at a later date depending upon convenience. Every effort was made to operate as early as possible and mobilized as early as possible. The average time between injury and operation was 5.7±3.8 days.
All patients were taken up for surgery when general condition was stable under general anesthesia or brachial block. The implants used were Recon plates, dynamic compression plate, distal humerus plate, 1/3 tubular plates and cancellous screws. The follow up period ranges between 20 weeks to 40 weeks with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks. For functional evaluation of the results Cassebaum’s scale has been chosen.
INCLUSION CRITERIA
1. Those patients who are above the age of 20 years and managed surgically were included in the study 2. Patients presenting with isolated distal humerus fractures with or without osteoporotic changes were included in the study. 3. Both closed and open distal humerus (Grade I & II) fractures were included in the study.
EXCLUSION CRITERIA
1. Children with distal humerus fractures in whom, growth plate is still open. 2. Patients lost in follow up. 3. Patients managed conservatively for other medical reasons. 4. Patients medically not fit for surgery. 5.Pathological fractures. 6. Incomplete and undisplaced fractures in adults. 7. Grade III compound fractures excluded.
SURGICAL PROCEDURES:
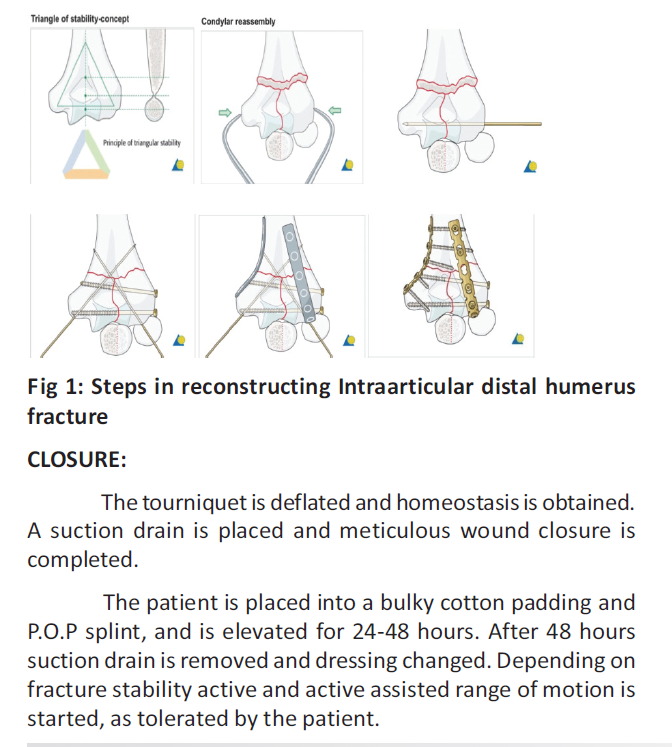
A straight posterior Campbell incision is used with slight radial deviation across the tip of the olecranon. The ulnar nerve is then identified and tagged with a vessel loop (umbilical tape). For adequate exposure of the distal condyles, an olecranon osteotomy is required. An intra-articular osteotomy is done after a predrilling of olecranon two or three drills, to avoid intraarticular comminution, because direct visualization of the articular surface is necessary for an exact anatomic reduction. A transverse or chevron intra articular osteotomy will be done. The osteotomy is completed with an osteotome used as lever to crack through the articular surface. Before the osteotomy, it is helpful to predrill the olecranon for the fixation preferred.
ANATOMIC REDUCTION AND STABLE FIXATION OF THE CONDYLES:
The first step is to anatomically reduce the articular surface; provisional stabilization can be accomplished with K wires or a bone holding forceps. Once this is accomplished, the condyles are held together with lag screw fixation. When there is no intra articular comminution, it is easier to drill from inside out through the capitellum to center the lag screw before anatomic reduction.
This will allow the lag screw to be in the proper position for optimal stabilization of the condyles. The condyles then are reduced and drilled from the capitellum into the trochlea. A 4mm cancellous screw then is placed, making sure the threads completely cross the fracture line. Those fractures with intra articular comminution are much more difficult. The intercondylar distance must be maintained, even in the face of the intracondylar comminution. The condyles are held together with a non-lag screw to prevent narrowing of the intercondylar distance. A defect between condyles then can be spanned by a corticocancellous bone graft. Additional, small articular fragments can be held in place with countersunk screws.
The next step is to anatomically reattach the condyles to the humeral shaft. Temporary fixation is achieved with crossed K wires. Stable fixation is achieved by using two plates or sometimes only one plate or multiple cancellous, cortical screws or simply k wires depending on stability that is achieved at surgery.
The ulnar or medial plate is placed along the medial surface of the distal humerus, and the radial or lateral plate is placed along the posterior surface of the distal humerus, or lateral border of the humerus.
This construct will provide optimal biomechanical stability. To avoid fixation failure before bone healing, a cancellous bone graft is recommended for bone defects and comminution and is placed at this time. The olecranon osteotomy then reduced and fixation applied, commonly used are either two k wires or 6.5mm cancellous screw each with tension band wire.
After adequate stable fixation has been achieved, the elbow is placed through a range of motion. If olecranon impingement limits extension, a portion of the tip maybe excised. It is important to assure that the olecranon and the coronoid fossae are not compromised by bone fragments or hardware.
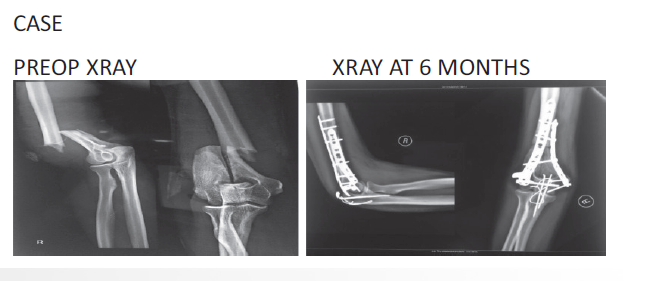
Followup & evaluation:
Post operative care included analgesia, limb elevation, antibiotics (ceftriaxone / amikacin and metrogyl) for three days. Primary dressing on second day. Physiotherapy which includes, finger movements at the time of discharge (on 3rd day). Slab applied for 10 days till suture removal and graded physiotherapy started after the suture removal. The check xray taken after 2 days and the follow up x-rays after 3 weeks , 3 months and final movement evaluation at 7 months. The follow up period ranges between 20 weeks to 40 weeks with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks. For functional evaluation of the results Cassebaum’s scale has been chosen.
THE RATING SYSTEM OF CASSEBAUM7
Excellent: Extension deficit of 15o or less and flexion to 130o or more Good: Extension deficit of 15o to 30o and flexion of 120o-130o Fair: Extension deficit of 30o- 40o and flexion to 90o-120o Poor: Extension deficit of 40o or more and flexion to less than 90o The data on elbow motion was combined with the patient’s subjective symptoms to provide an overall functional rating. An excellent rating was given for a symptom free elbow with a normal or nearly normal range of motion, a good overall rating for good or excellent elbow motion with some subjective symptoms; a fair rating for a fair range of motion of the elbow with or without symptoms; and a poor rating for both limited mobility and limited function.
COMPLICATIONS
No surgery is without complications, like wise complications do occur with surgery of intercondylar fractures also. These include: 1. Neurogenic: Radial nerve/ ulnar nerve palsy 2. Heterotopic ossification. 3. Infection 4. Non union 5. Failure of fixation 6. Soft tissue injury 7. Elbow deformity due to incongruent growth 8. Sudeck’s dystrophy 9. Hardware pain 10. Olecranonosteotomy nonunion.
 EVALUATION:
Outcome of management of distal humerus fractures
in adults was evaluated using Cassebaum scale. It was observed
that 47 % cases presented with excellent outcome, 30 % cases
presented with good outcome, 20 % cases presented with fair
outcome, 3 % cases presented with poor outcome.
EVALUATION:
Outcome of management of distal humerus fractures
in adults was evaluated using Cassebaum scale. It was observed
that 47 % cases presented with excellent outcome, 30 % cases
presented with good outcome, 20 % cases presented with fair
outcome, 3 % cases presented with poor outcome.
 DISCUSSION:
DISCUSSION:
Fractures of the distal humerus in adults are difficult to treat because of their rarity and associated significant comminution. The results of managing these fractures nonoperatively are limited by failure to get anatomical reduction and early mobilization, which often results in painful stiff elbow and/or pseudarthrosis. Hence an operative management with anatomical reduction of the fragments becomes the treatment of choice for these fractures1. The management of intercondylar and comminuted intra-articular distal humerus fractures has been controversial.
The critical factors for successful outcome remain those advocated earlier by Cassebaum5, 6. These include meticulous surgical technique, stable internal fixation, and early controlled post-operative mobilization. The careful identification and temporary fixation of the articular fragments with Kirschner wires enables the surgeon to accurately assess the anatomy of individual fracture and to tailor the placement and type of internal fixation to meet each fracture’s unique requirements.
The trans-olecranon approach with the patient in lateral position offers excellent approach of the articular surface and distal end of humerus without the soft tissue trauma, this approach also facilitates identification and protection of ulnar nerve. The classification system of Muller’s et al (AO) is used in this study because it is well suited for operative conditions. The rating system of Cassebaum has been adopted for use in this study. All the fractures were reduced to maintain articular surface and fixed with K wires, cancellous/Cannulated cancellous screws, 3.5mm plates along with tension band wire or cancellous screw fixation for olecranon osteotomy. At followup, patients were assessed clinically and radiologically. In the present study the average age was 47.33 years, the female/ male ratio 18:12 of the 30 cases taken up for study, all were followed up. Those cases that didn’t turn up for follow up were not included in the study. Accidental falls were the main cause of most of the fractures in older age group while Road Traffic Accidents (RTA) is the main cause in younger individuals. The complication rate in present study is 20%. Henley et al reported 4% superficial infection 7% of ulnar neuropathy, 5% of implant failure, 2% of non-union and 4% incidence of heterotrophic ossification. Kundel et al reported 10% of superficial infection and pain, 22% of ulnar neuropathy, 10% non-union, 6% pain.
Outcome of surgical management of distal humerus fractures in adults by open reduction and interal fixation was evaluated using Cassebaum scale it was observed that 47 % cases presented with excellent outcome, 30 % cases presented with good outcome, 20 % cases presented with fair outcome, 1 % cases presented with poor outcome.
Most of the patients with fair results were either associated with other fractures of same upper limb or had osteopenic bones which prevented them from early postoperative mobilization which was the reason for the fair results. The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable in restoring articular surface and early rehabilitation which decreases the morbidity and resulting in good functional outcome.
CONCLUSION:
Most of Distal humerus fractures are extra articular fractures which demands careful evaluation, classification of fracture type and pre- operative planning. Operative treatment with rigid anatomical internal fixation should be the line of treatment for extra articular and intercondylar fractures, more so in young adults as it gives best chance to achieve good elbow function. During open reduction & internal fixation, anatomical restoration of articular surface should be given prime importance. Early post-operative mobilisation by active assisted exercises and physiotherapy is must for good functional outcome. The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable, in restoring articular surface and early rehabilitation which decreases morbidity, resulting good functional outcome. Single column fixation of extra articular distal humerus fractures by precontoured distal humerus locking plates also yielded excellent outcome in our study.
REFERENCES:
1. Gupta R- Intercondylar fractures of distal humerus in adults.Injury. 1996 Oct; 27(8):569- 72.
2. Rockwood & Green's Fractures in Adults, 6th Edition Copyright ©2006 Lippincott Williams & Wilkins
3. Jupiter JB, Morrey BF. Fractures of the distal humerus in the adult: The elbow and its disorders, 2nd ed. Philadelphia: WB Saunders, 1993:328â•“366
4. Watson–Jones R: Fractures and joint injuries Wilson Elsevier 2009: 7th edition.
5. Cassebaum WH: Operative treatment of T and Y Fractures of lower end of humerus, Am J Surg. 1952 Mar; 83(3):265- 70.
6. Orthopedic Trauma Association Committee for Coding and Classification. OTA Coding and Classification Committee.Fracture and dislocation compendium.J Orthop Trauma 1996; 10[Suppl 1]:154.
7. Cassebaum WH: Open reduction of T and Y Fractures of lower end of humerusJ Trauma. 1969 Nov; 9(11):915-25.
How to cite this article : Koneru Rao T, Nagendra Babu M, Karthik Reddy M, Krishna Kumar V.A study of distal humerus fractures in adults by open reduction and internal fixation. . Perspectives in Medical Research 2019; 7(2):26-30
Sources of Support: Nil,Conflict of interest:None declared
Year : 2019 | Volume : 7 | Issue : 2 Page : 26-30
Koner Rao T1, Nagendra Babu M2, Karthik Reddy R3, Krishna Kumar V4
1Associate professor, 2Professor & HOD, Department of Orthopaedics, 3, 4Post graduate student, Prathima
Institute of Medical Sciences, Karimnagar, Telangana, India.
*Address for correspondence:: DR. T. Koneru Rao, Associate professor, Department of Orthopedics, Prathima Institute of
Medical Sciences, Karimnagar, Telangana, India.
Distal humerus fractures represent one of the most complicated and challenging fractures in the upper extremity. Distal humerus fractures in adults are difficult fractures to treat because of significant comminution and they are rare fractures which prevents the individual surgeon from accumulating sufficient personal experience to critically evaluate the results of the treatment.
Aims & Objectives:
1. To evaluate the role of operative management in distal humerus fractures. 2. To follow up & evaluate results on patients operated upon and note the functional outcome and complications.
Patients and Methods:
The present study is a prospective study of 30 cases of Distal humerus fractures (AO Type 13.A, 13.B and 13.C, 12 male and 18 females, age ranging from 20 to 70) treated by open reduction and internal fixation over two years, from September 2016 to August 2018 was conducted in department of orthopaedics, Prathima institute of medical sciences, Karimnagar. All patients were selected among admissions, operated and results were assessed clinically and radiographically. The functional evaluation of the results Cassebaum’s scale has been chosen. The follow up period ranges with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks and complications noted.
Results:
Outcome of surgical management of distal humerus fractures in adults by open reduction and interal fixation was evaluated using Cassebaum scale it was observed that 47% cases presented with excellent outcome, 30% cases presented with good outcome, 20% cases presented with fair outcome, 1% cases presented with poor outcome. In the present study 7% patients had superficial wound infections with hardware pain and 7% patients had presented with hardware pain and 3% delayed union 3% ulnar neuropathy, respectively.
Conclusion:
The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable, in restoring articular surface and early rehabilitation which decreases morbidity, resulting good functional outcome. Keywords:
distal humerus fracture, Cassebaum’s scale, open reduction and internal fixation, dual plates, AO: Arbeitsgemeinschaft Fur Osteosynthesefragen. INTRODUCTION
Distal humerus fractures represent one of the most complicated and challenging fractures in the upper extremity. Distal humerus fractures in adults are difficult fractures to treat because of significant comminution and they are rare fractures which prevents the individual surgeon from accumulating sufficient personal experience to critically evaluate the results of the treatment. The results of managing these fractures nonoperatively are limited by failure to get anatomical reduction and early mobilization, which often results in painful stiff elbow and/or pseudarthrosis. Hence an operative management with anatomical reduction of the fragments becomes the treatment of choice for these fractures1. The complex three-dimensional geometry of the distal humerus poses a considerable challenge to reconstruction2.
The distal humerus fractures are rare fractures constituting 2%3 of all body fractures. Watson and Jones4 wrote “few fractures are more difficult to treat” while describing them, thus describing their complexity. The forearm musculature originating on the condyles tends to produce rotational displacement even when closed reduction is achieved. The only reliable method for restoring the normal alignment and contour of the distal humerus is operative exposure and direct manipulation of fracture fragments. However, fixation of fracture fragments must be stable enough to allow motion while ensuring union. In most cases open reduction with stable rigid internal fixation is required to fulfil the above goal.
The recommendations for treatment have ranged widely from essentially no treatment to operative reduction and extensive internal fixation. In some of these fractures particularly those with intra articular comminution, anatomical restoration of the articular surface cannot be adequately achieved or maintained through manipulative reduction alone.
Critics of open reduction have argued that the additional surgical trauma and the inherent difficulty in securely stabilizing the small intra articular fragments will lead to added fibrosis and a less satisfactory result. Even those who have recommended operative treatment differ widely in their opinions with regard to extent, approach, type of internal fixation to be used and when to start the post-operative mobilization.
The recent trend has been immediate open reduction, stable and rigid internal fixation and early post-operative mobilization. The anatomic complexity of distal humerus makes surgical reconstruction difficult. The fabrication of newer implants however, has increased the reliability of the operative stabilization, while placing additional demands on the surgeon expertise.
Injuries of the elbow lead to chronic pain and permanent restriction of motion, limiting the use of hand in basic daily activities from eating to personal hygiene require a wide range of positions and movements at the elbow in flexion, extension and forearm rotation. Recent advances in surgical techniques and equipment designed to make possible rigid osteosynthesis of smaller intra articular fragments which permits early post-operative rehabilitation and achieve improved results.
Patients and Methods:
A prospective study to evaluate the role of open reduction and internal fixation in the treatment of distal humerus fractures. Patients selected for this operation were of different ages and genders, admitted and treated in Prathima Institute of Medical Sciences, Karimnagar during the years 2016-2018. The classification criteria used was AO classification in which most of them were AO type 13.A and remaining were AO type 13.B and AO type 13.C
A thorough general examination and local examination was performed. Radiological examination of the part and routine investigations were carried out. Patients were taken up for surgery as early as possible in all the cases. Old people with medical problems after thorough work up were taken up once the patient is fit for surgery. Pre operatively all patients were immobilized in above elbow plaster of paris slab with elevation of limb. Associated injuries were dealt simultaneously or at a later date depending upon convenience. Every effort was made to operate as early as possible and mobilized as early as possible. The average time between injury and operation was 5.7±3.8 days.
All patients were taken up for surgery when general condition was stable under general anesthesia or brachial block. The implants used were Recon plates, dynamic compression plate, distal humerus plate, 1/3 tubular plates and cancellous screws. The follow up period ranges between 20 weeks to 40 weeks with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks. For functional evaluation of the results Cassebaum’s scale has been chosen.
INCLUSION CRITERIA
1. Those patients who are above the age of 20 years and managed surgically were included in the study 2. Patients presenting with isolated distal humerus fractures with or without osteoporotic changes were included in the study. 3. Both closed and open distal humerus (Grade I & II) fractures were included in the study.
EXCLUSION CRITERIA
1. Children with distal humerus fractures in whom, growth plate is still open. 2. Patients lost in follow up. 3. Patients managed conservatively for other medical reasons. 4. Patients medically not fit for surgery. 5.Pathological fractures. 6. Incomplete and undisplaced fractures in adults. 7. Grade III compound fractures excluded.
SURGICAL PROCEDURES:
A straight posterior Campbell incision is used with slight radial deviation across the tip of the olecranon. The ulnar nerve is then identified and tagged with a vessel loop (umbilical tape). For adequate exposure of the distal condyles, an olecranon osteotomy is required. An intra-articular osteotomy is done after a predrilling of olecranon two or three drills, to avoid intraarticular comminution, because direct visualization of the articular surface is necessary for an exact anatomic reduction. A transverse or chevron intra articular osteotomy will be done. The osteotomy is completed with an osteotome used as lever to crack through the articular surface. Before the osteotomy, it is helpful to predrill the olecranon for the fixation preferred.
ANATOMIC REDUCTION AND STABLE FIXATION OF THE CONDYLES:
The first step is to anatomically reduce the articular surface; provisional stabilization can be accomplished with K wires or a bone holding forceps. Once this is accomplished, the condyles are held together with lag screw fixation. When there is no intra articular comminution, it is easier to drill from inside out through the capitellum to center the lag screw before anatomic reduction.
This will allow the lag screw to be in the proper position for optimal stabilization of the condyles. The condyles then are reduced and drilled from the capitellum into the trochlea. A 4mm cancellous screw then is placed, making sure the threads completely cross the fracture line. Those fractures with intra articular comminution are much more difficult. The intercondylar distance must be maintained, even in the face of the intracondylar comminution. The condyles are held together with a non-lag screw to prevent narrowing of the intercondylar distance. A defect between condyles then can be spanned by a corticocancellous bone graft. Additional, small articular fragments can be held in place with countersunk screws.
The next step is to anatomically reattach the condyles to the humeral shaft. Temporary fixation is achieved with crossed K wires. Stable fixation is achieved by using two plates or sometimes only one plate or multiple cancellous, cortical screws or simply k wires depending on stability that is achieved at surgery.
The ulnar or medial plate is placed along the medial surface of the distal humerus, and the radial or lateral plate is placed along the posterior surface of the distal humerus, or lateral border of the humerus.
This construct will provide optimal biomechanical stability. To avoid fixation failure before bone healing, a cancellous bone graft is recommended for bone defects and comminution and is placed at this time. The olecranon osteotomy then reduced and fixation applied, commonly used are either two k wires or 6.5mm cancellous screw each with tension band wire.
After adequate stable fixation has been achieved, the elbow is placed through a range of motion. If olecranon impingement limits extension, a portion of the tip maybe excised. It is important to assure that the olecranon and the coronoid fossae are not compromised by bone fragments or hardware.
Followup & evaluation:
Post operative care included analgesia, limb elevation, antibiotics (ceftriaxone / amikacin and metrogyl) for three days. Primary dressing on second day. Physiotherapy which includes, finger movements at the time of discharge (on 3rd day). Slab applied for 10 days till suture removal and graded physiotherapy started after the suture removal. The check xray taken after 2 days and the follow up x-rays after 3 weeks , 3 months and final movement evaluation at 7 months. The follow up period ranges between 20 weeks to 40 weeks with average of 7 months and patients were assessed for functional capacity and radiological fracture healing capacity periodically every 4 – 6 weeks. For functional evaluation of the results Cassebaum’s scale has been chosen.
THE RATING SYSTEM OF CASSEBAUM7
Excellent: Extension deficit of 15o or less and flexion to 130o or more Good: Extension deficit of 15o to 30o and flexion of 120o-130o Fair: Extension deficit of 30o- 40o and flexion to 90o-120o Poor: Extension deficit of 40o or more and flexion to less than 90o The data on elbow motion was combined with the patient’s subjective symptoms to provide an overall functional rating. An excellent rating was given for a symptom free elbow with a normal or nearly normal range of motion, a good overall rating for good or excellent elbow motion with some subjective symptoms; a fair rating for a fair range of motion of the elbow with or without symptoms; and a poor rating for both limited mobility and limited function.
COMPLICATIONS
No surgery is without complications, like wise complications do occur with surgery of intercondylar fractures also. These include: 1. Neurogenic: Radial nerve/ ulnar nerve palsy 2. Heterotopic ossification. 3. Infection 4. Non union 5. Failure of fixation 6. Soft tissue injury 7. Elbow deformity due to incongruent growth 8. Sudeck’s dystrophy 9. Hardware pain 10. Olecranonosteotomy nonunion.
EVALUATION:
Outcome of management of distal humerus fractures
in adults was evaluated using Cassebaum scale. It was observed
that 47 % cases presented with excellent outcome, 30 % cases
presented with good outcome, 20 % cases presented with fair
outcome, 3 % cases presented with poor outcome.
DISCUSSION:Fractures of the distal humerus in adults are difficult to treat because of their rarity and associated significant comminution. The results of managing these fractures nonoperatively are limited by failure to get anatomical reduction and early mobilization, which often results in painful stiff elbow and/or pseudarthrosis. Hence an operative management with anatomical reduction of the fragments becomes the treatment of choice for these fractures1. The management of intercondylar and comminuted intra-articular distal humerus fractures has been controversial.
The critical factors for successful outcome remain those advocated earlier by Cassebaum5, 6. These include meticulous surgical technique, stable internal fixation, and early controlled post-operative mobilization. The careful identification and temporary fixation of the articular fragments with Kirschner wires enables the surgeon to accurately assess the anatomy of individual fracture and to tailor the placement and type of internal fixation to meet each fracture’s unique requirements.
The trans-olecranon approach with the patient in lateral position offers excellent approach of the articular surface and distal end of humerus without the soft tissue trauma, this approach also facilitates identification and protection of ulnar nerve. The classification system of Muller’s et al (AO) is used in this study because it is well suited for operative conditions. The rating system of Cassebaum has been adopted for use in this study. All the fractures were reduced to maintain articular surface and fixed with K wires, cancellous/Cannulated cancellous screws, 3.5mm plates along with tension band wire or cancellous screw fixation for olecranon osteotomy. At followup, patients were assessed clinically and radiologically. In the present study the average age was 47.33 years, the female/ male ratio 18:12 of the 30 cases taken up for study, all were followed up. Those cases that didn’t turn up for follow up were not included in the study. Accidental falls were the main cause of most of the fractures in older age group while Road Traffic Accidents (RTA) is the main cause in younger individuals. The complication rate in present study is 20%. Henley et al reported 4% superficial infection 7% of ulnar neuropathy, 5% of implant failure, 2% of non-union and 4% incidence of heterotrophic ossification. Kundel et al reported 10% of superficial infection and pain, 22% of ulnar neuropathy, 10% non-union, 6% pain.
Outcome of surgical management of distal humerus fractures in adults by open reduction and interal fixation was evaluated using Cassebaum scale it was observed that 47 % cases presented with excellent outcome, 30 % cases presented with good outcome, 20 % cases presented with fair outcome, 1 % cases presented with poor outcome.
Most of the patients with fair results were either associated with other fractures of same upper limb or had osteopenic bones which prevented them from early postoperative mobilization which was the reason for the fair results. The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable in restoring articular surface and early rehabilitation which decreases the morbidity and resulting in good functional outcome.
CONCLUSION:
Most of Distal humerus fractures are extra articular fractures which demands careful evaluation, classification of fracture type and pre- operative planning. Operative treatment with rigid anatomical internal fixation should be the line of treatment for extra articular and intercondylar fractures, more so in young adults as it gives best chance to achieve good elbow function. During open reduction & internal fixation, anatomical restoration of articular surface should be given prime importance. Early post-operative mobilisation by active assisted exercises and physiotherapy is must for good functional outcome. The concept of open reduction and internal fixation of fractures of the distal humerus with dual plates is very valuable, in restoring articular surface and early rehabilitation which decreases morbidity, resulting good functional outcome. Single column fixation of extra articular distal humerus fractures by precontoured distal humerus locking plates also yielded excellent outcome in our study.
REFERENCES:
1. Gupta R- Intercondylar fractures of distal humerus in adults.Injury. 1996 Oct; 27(8):569- 72.
2. Rockwood & Green's Fractures in Adults, 6th Edition Copyright ©2006 Lippincott Williams & Wilkins
3. Jupiter JB, Morrey BF. Fractures of the distal humerus in the adult: The elbow and its disorders, 2nd ed. Philadelphia: WB Saunders, 1993:328â•“366
4. Watson–Jones R: Fractures and joint injuries Wilson Elsevier 2009: 7th edition.
5. Cassebaum WH: Operative treatment of T and Y Fractures of lower end of humerus, Am J Surg. 1952 Mar; 83(3):265- 70.
6. Orthopedic Trauma Association Committee for Coding and Classification. OTA Coding and Classification Committee.Fracture and dislocation compendium.J Orthop Trauma 1996; 10[Suppl 1]:154.
7. Cassebaum WH: Open reduction of T and Y Fractures of lower end of humerusJ Trauma. 1969 Nov; 9(11):915-25.
How to cite this article : Koneru Rao T, Nagendra Babu M, Karthik Reddy M, Krishna Kumar V.A study of distal humerus fractures in adults by open reduction and internal fixation. . Perspectives in Medical Research 2019; 7(2):26-30
Sources of Support: Nil,Conflict of interest:None declared

Open Access
Perspectives in Medical Research is committed to keeping research articles Open Access.Journal permits any users to read, download, copy, print, search, or link to the full texts of these articles...
Read more
© PIMR.org.in - 2013. All Rights Reserved.