
Femur shaft fracture treatment in school-aged children using titanium elastic nails
Abstract
INTRODUCTION: Titanium elastic nails are used to treat femur shaft fractures in paediatric patients. This method is minimally invasive and does not cause epiphyseal injury or impairment of femoral head blood supply.
OBJECTIVES: The objective is to evaluate the results of operative treatment of femur shaft fractures in the age group between 6 and 16 years with titanium elastic nailing system (TENS), using Flynn’s criteria.
METHODS: This prospective clinical study was conducted during the period from November 2018 to November 2020. Thirty cases were treated with mean follow up of 12 months.
RESULTS: The final outcome was excellent in 21 cases, satisfactory in 6 cases and there were 3 poor outcome cases. Eight patients had limb length discrepancy varying from 0.5-2cm. Five patients had skin irritation, 3 patients had angular mal-union and 1 patient had persistent pain with skin breakdown. None of the patient had infection, rotational mal-union, delayed or non union.
CONCLUSION: Titanium elastic nail fixation is a simple, easy and effective method for management of paediatric femur fracture between 6 and 16 years age. With this method of treatment, careful consideration to patient’s age and body weight should be given to prevent the poor result.
Keywords
Femur shaft fracture, Pediatric, titanium elastic nails
INTRODUCTION
Femoral shaft fractures constitute 1.4% to 1.7% of all pediatric fractures 1, 2 . Children up to 5 years of age with this fracture are treated with hip spica cast and those nearing skeletal maturity are treated with interlocking intramedullary nailing. In 6-16years old children, closed reduction and hip spica application, open reduction and plating, external fixation and titanium elastic nailing system (TENS) are the different treatment methods used by orthopedic surgeons. So there is no uniform agreement regarding the treatment of femoral shaft fracture in school-aged children (6years to16years).
When femur shaft fracture is treated with conservative methods, school-aged children have a high risk of shortening and malunion. In addition, the problems of transportation, cast intolerance by the child and keeping the child clean are encountered by the family, in caring for a child in a spica cast 3 .Plate application demands extensive dissection and periosteal stripping. Pin tract infection and delayed union are well known with External fixation 4 . Standard rigid intramedullary nails require insertion at or near the piriformis fossa, and the use of these implants in skeletally immature patients has led to iatrogenic femoral head ischemic necrosis 5 . Whatever the method of treatment, the goals should be to stabilize the fracture, to control length and alignment, to promote bone healing, and to minimize the morbidity and complications for the child and family 6 .
Treatment of pediatric fractures dramatically changed in the 1980s, when pediatric orthopedic surgeons from Nancy, France, developed the technique of elastic stable intramedullary nailing (ESIN) using titanium nails 7 . Compared to other methods, TENS represents an amalgamation of conservative and surgical treatment techniques. The purpose of this study is to report our experience of treating femoral shaft fracture in school-aged children by closed reduction and internal fixation with titanium elastic nails, using Flynn’s criteria 8 .
METHODS
This prospective clinical study was conducted from November 2018 to May 2020. Ethical committee clearance was taken. We included 30 children in the 6 to 16 years age group with femoral shaft fractures admitted in our institution by convenience sampling for our study. Polytrauma, Compound fractures (grade 3), metaphyseal fractures and pathological fractures associated with malignant tumor of the femur were excluded.
Written informed consent was taken from the parents of the patients who participated in the study. Relevant history and examination findings were noted. Plain radiographs of antero-posterior and lateral views of the thigh including hip and knee joints were assessed during pre-operative planning to note the fracture personality and diameter of the femoral canal at the isthmus.
SURGICAL TECHNIQUE:
A traction table was used in all patients. Two TENS nails of equal diameter, which together fill 80% of the narrowest canal diameter were selected. A gentle 30-degree bend was placed in the nail in such a way that the maximum curvature would be at the level of the fracture. Nails were introduced in a retrograde direction in all patients. Distal physis was identified by fluoroscopy, and its location was marked on the skin. A 2 cm longitudinal skin incision was made over the medial and lateral surface of the distal thigh. A hemostat was used to split the soft tissue down to the bone. An opening was made in the cortex using a 3.2mm drill bit, 2.5 cm proximal to the distal femoral growth plate.
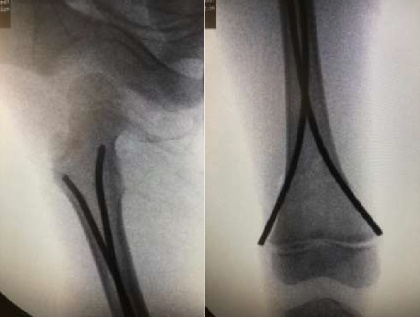
Under image intensifier control, the pre-contoured nail was driven by toggling or with back and forth reciprocating movement or with a help of a hammer up to the fracture site. The reduction was gained by giving traction and manipulation at the fracture site. A nail was introduced into the medullary canal of the proximal fragment. The second pre-contoured nail was advanced to enter the canal of the proximal fragment and in the meantime, traction was released to avoid distraction. Then, both nails were pushed further till their tips became fixed into the cancellous bone of the proximal femoral metaphysis. The double C construct with maximum curvature at the fracture level ensures 3-point fixation. The tip of the nail that entered the lateral femoral cortex was inserted just distal to the trochanteric epiphysis. The opposite nail introduced from the medial side was inserted up to the same level towards the calcar region[Figure 1] .Distally the nails were cut leaving about 1.5 to 2cm outside the bone. The nails were not bent and allowed to lie flush with the bone surface[Figure 1].
Postoperatively, an Above Knee (high groin) slab was applied. Post-operative Anteroposterior and Lateral radiographs of the full-length femur were taken on the next day. Patients were advised strict non-weight bearing at the time of discharge. At 2 weeks, the slab was replaced by a knee Immobilizer brace in compliant patients, and patients were encouraged to do knee bending exercise. Weight-bearing as tolerated, was allowed after soft callus was noted in the radiograph at around 3-6 weeks. The patient was followed up at 2 weeks, 4 weeks, 6 weeks, 3 months, and 6 months. Observations were made regarding fracture union, range of motion at the knee joint, limb length discrepancy, rotatory and angular deformity.
RESULTS
Out of 30 patients, 22 (73%) were boys and 8 (27%) were girls. Twenty-one (70%) patients had right-sided involvement and 9(30%) patients had left-sided involvement. There was a history of Road traffic accident in 23 (77%) patients and fall in 7 (23%) patients. The mean age of the patients was 10.7 years and the mean weight was 31.8 kgs (21-52 kgs). The level of fracture was at the middle third in 20 patients; at the upper third in 7 patients and at the lower third of shaft femur in 3 patients. Twelve patients had oblique, 10 patients had spiral and 8 patients had transverse fracture patterns. The mean time interval between admission and surgery was 4.5days. The average duration of surgery was 55 minutes. The mean radiological time to union was 10 weeks. The fracture was considered united when bridging callus was seen in at least 3 out of 4 cortices. The mean follow-up period was 12 months (6-18 months). All patients were full weight-bearing at 6 months follow up.
At the end of 6 months, results were assessed using Flynn’s criteria 8 . Twenty-one (70%) patients had excellent results [ Figure 2 ], 6(20%) patients had satisfactory results, and 3(10%) patients had poor results.
Eight patients had limb length discrepancy varying from 0.5-2cm. Only one patient had a 2cm shortening. Five patients had skin irritation, 3 patients had angular mal-union and 1 patient had persistent pain with skin breakdown. None of the patients had an infection, rotational malunion, delayed or nonunion.
|
Patient |
Age |
Sex |
Weight (kg) |
Mode of injury |
Side |
Pattern of fracture |
Level of fracture |
Radiological Time for union (weeks) |
limb length discrepancies |
mal alignment |
persistent pain |
Other complications |
|
1 |
13 |
M* |
42 |
RTA† |
Left |
Transverse |
Middle third |
13 |
-- |
Anterior angulation 15 degree |
-- |
-- |
|
2 |
14 |
M |
38 |
RTA |
Right |
Spiral |
Lower Third |
10 |
-- |
valgus 15 degree |
-- |
-- |
|
3 |
16 |
M |
50 |
RTA |
Left |
Oblique |
Middle third |
16 |
2 cm shortening |
-- |
present |
skin break down |
(M*-Male,RTA†- Road Traffic Accident)


DISCUSSION
According to Moroz et al 9 , the ideal patient for flexible intramedullary nailing is the child between the ages of 5 and 11 years old with a length-stable femur fracture, in the mid-80% of the diaphysis, who has a bodyweight less than 50 kg. An in-vitro biomechanical study 10 concluded that patients weighing more than 40 to 45 kg who undergo stabilization of a transverse midshaft femur fracture with two 4mm titanium elastic nails are at risk of loss of reduction in the sagittal and coronal planes.
Ulici et al 11 , conducted a retrospective study on 137 patients with femoral shaft fractures treated by elastic stable intramedullary nailing. Patients’ age ranged between 4 and 17 years. Complications occurred in 29 patients (21%) and consisted of delayed union, axial deformities, or lower limb length discrepancies. They concluded that the mechanism of injury, age >11 years and weight > 50 kg, with the mechanism of injury (high-velocity trauma) being the most important and the only independent predictor for the development of complications such as delayed union or deformity.
Patients with femoral shaft fractures treated with TEN and a minimum 6 months follow-up were included in a retrospective review by Siddiqui et al 12 . Femur fractures were categorized into 2 groups: length unstable (spiral, comminuted, or long oblique fractures) versus length stable (transverse and short oblique). Complications and reoperations were compared between the groups. A total of 57 patients with 58 femoral shaft fractures were included. The mean age was 5 (1 to 11) years and the mean follow-up was 20.4 (6.0 to 81.2) months. The mean weight was 22.9 (11.0 to 40.5) kg. The main finding of this study was that, there was no significant difference in outcomes or complications between length stable and length unstable femoral shaft fractures treated with TEN.
A multicenter study conducted by Memeo et al 13 , involved 62 patients of both sexes, between 6 and 14 years of age, with closed femoral shaft fractures. The commonest complication observed was pain at the nail entry point (24.19%) due to a local inflammatory reaction.
Studies 9, 10, 11 have shown that age and weight of the child are important determinants of the outcome in pediatric femoral shaft fractures. The remodeling capacity of the fracture depends on the age of the child. The younger the age, the greater is the remodeling capacity. The stress to which the implant is subjected depends on the weight of the child. Heavier the child, the titanium nails can bend leading to loss of reduction, malunion, or reoperation. It was observed that the bodyweight of our patients was either appropriate for age or was underweight 14 . None of the children was obese.
Regarding poor outcome in our study , one patient did early full weight-bearing which resulted in malunion (15-degree anterior angulation). The second patient had 15-degree valgus malunion. The third patient developed a 2cm shortening due to an unstable (long oblique) fracture pattern resulting in a prominent nail end. He subsequently developed persistent pain with skin breakdown[Figure 3] resulting in implant removal at 8 months. The 3 patients with poor results had a road traffic accident and were >11 years of age with body weight close to or above 40 kg.
In our study, long-standing skin irritation by nail end was seen in 5(16.66%) patients, which was the most common complication. Terminal restriction of flexion due to pain interfered with squatting. These patients gained back full range of movements at the knee joint, after implant removal.
TENS is based on a 3-point fixation where the deforming muscular forces are balanced by two opposing flexible nails. According to Flynn et al 8 , “The ideal device to treat pediatric femur fractures would be a simple, load-sharing internal splint allowing mobilization and maintenance of alignment for a few weeks until bridging callus forms. The device would exploit a child’s denser bone, rapid healing, and ability to remodel, without risking the physes or blood supply to the femoral head”.
We are convinced that TENS has the above-mentioned features. In addition, it is easy to implant and easy to remove with minimum morbidity to the patient. The surgical technique has a short learning curve and requires minimal inventory.
The short-term follow-up period and less number of patients are the limitations of our study. Literature is available about the use of lateral entry antegrade intramedullary locking nail for treating paediatric femoral shaft fractures 15, 16 . They avoid using piriformis fossa entry site, but use a very lateral trochanteric entry point therby reducing the risk of osteonecrosis. We admit that we have no experience of using such devices.
CONCLUSION
TENS is a simple, safe, rapid, and biological method of treating femoral shaft fractures in school-aged children (from 6 years to 16 years old). One should give careful consideration to the patient's age and weight to prevent poor results. It is prudent to delay weight-bearing till the fracture unites, in older and heavier children.

