SciresolSciresolhttps://jmsh.ac.in/Journal of Medical Sciences and Health10.47799/pimr.1401.26.7CASE REPORT<p><em>Ascaris lumbricoides</em> through a Pigtail Catheter: A Case Report of Liver Abscess</p>303202620261411Abstract
<p><emphasis>Ascaris lumbricoides</emphasis> infection is common in tropical and subtropical countries, but hepatic abscess due to ascariasis is rare. We report a case of an 80-year-old female who presented with abdominal pain and breathlessness. Ultrasonography revealed a large abscess in the right lobe of the liver, and a USG-guided pigtail catheter was inserted. Chocolate brown pus was drained, and microbiological examination was negative. Subsequently, an adult <emphasis>A. lumbricoides</emphasis> worm was observed emerging through a pigtail catheter into the drainage bag. Stool examination did not show ova. Despite treatment, the patient succumbed to sepsis with acute respiratory distress syndrome and multiple organ dysfunction. This case highlights a rare presentation of hepatic ascariasis and underscores the importance of heightened clinical awareness.</p>
Keywords<I>Ascaris lumbricoides</I>Liver abscessPigtail catheterJagarwalKalyani1 PG Student, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Assistant Professor, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of General Surgery BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra IndiaWabaleVaishali2 PG Student, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Assistant Professor, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of General Surgery BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra IndiaBhoirLata3 PG Student, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Assistant Professor, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of General Surgery BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra IndiaKaryakarteRajesh4 PG Student, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Assistant Professor, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of General Surgery BJGMC & SGH Pune-411001, Maharashtra India Professor and Head, Department of Microbiology BJGMC & SGH Pune-411001, Maharashtra IndiaINTRODUCTION
Ascaris lumbricoides, a human roundworm, is the most common helminthic infection in the world [1], mainly affecting tropical and subtropical countries including India [2]. Transmission typically occurs through ingestion of embryonated eggs from the contaminated soil, food, and water [2].
Ascariasis, caused by A. lumbricoides, presents in acute and chronic forms. Acute manifestations, in the form of hypersensitivity reactions, result from larval migration through the lungs. While the complications due to adult worm include biliary obstruction, liver abscess, intestinal obstruction, and acute pancreatitis [3]. Chronic ascariasis is associated with impaired digestion and absorption, potentially leading to malnutrition[3].
Liver abscesses are most commonly attributed to Entamoeba histolytica, followed by pyogenic bacteria, and less frequently by Mycobacterium tuberculosis[4]. The emergence of an Ascaris worm through a pigtail catheter is a rare clinical occurrence, highlighting an unusual complication of ascariasis in the context of intrahepatic abscess.
CASE REPORT
An 80-year-old female presented to the surgical casualty department with complaints of abdominal pain for 10 days. The pain was insidious in onset and gradually progressive, accompanied by episodes of nausea and vomiting. She also reported breathlessness for the past 2–3 days. There was no history of any associated co-morbidities.
On general examination, the patient appeared well-nourished, afebrile, and haemodynamically stable. Blood sugar levels were within normal limits. Her SpO2 on room air was 90%, displaying fluctuations; therefore, she was administered oxygen intermittently via mask, maintaining O2 saturation at 98%. She was conscious and oriented. Respiratory examination revealed bilateral basal crackles with wheezing. Abdominal examination showed a soft abdomen with mild tenderness in the right hypochondriac region, but no hepatomegaly.
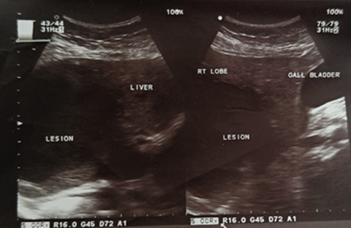
Chest X-ray demonstrated blunting of the costophrenic angles. Ultrasound of the thorax revealed free fluid in both pleural cavities, with minimum thicknesses of 5 mm and 7 mm in the right and left pleural cavities, respectively, suggestive of bilateral minimal pleural effusion. Abdominal ultrasound showed a liver of normal size and shape but showed a fairly-defined heterogeneous hypoechoic lesion in the right lobe of the liver, measuring 9.2 × 8.3 × 8.2 cm [Fig. 1], with minimal vascularity on colour Doppler. The portal vein and common bile duct were normal in course and calibre, and other abdominal structures appeared unremarkable. These findings were suggestive of an infective aetiology, likely a developing abscess in the right lobe of the liver.
Fig. 1: Abdominal ultrasound image showing lesion in the right lobe of the liver
The patient was admitted to the ward with a provisional diagnosis of amoebic liver abscess, and empirical management was initiated with intravenous metronidazole, ciprofloxacin, corticosteroids, and supportive care. Laboratory investigations revealed haemoglobin of 9.1 g/dL, total leucocyte count of 11,960/cumm (neutrophils 83.8%, lymphocytes 10.7%, monocytes 5.2%, eosinophils 0.1%, basophils 0.2%), and platelet count of 3,38,000/cumm. Liver and renal function tests were within normal limits for her age. Tests for HIV, HBsAg, and anti-HCV antibodies were negative.
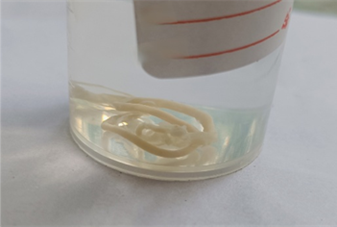
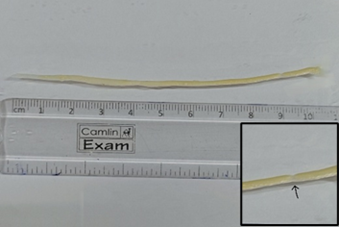
A USG-guided pigtail catheter was inserted into the liver abscess and left in situ. Chocolate brown-coloured frank pus was aspirated and sent to the microbiology laboratory [Fig. 2]. Wet mount examination did not reveal amoebic trophozoites, and bacterial culture showed no growth. On the day following pigtail catheter insertion, a worm was observed emerging through the catheter into the drainage bag as a coiled membranous structure. Gross examination of the macerated parasite revealed a whitish organism, measuring 10 cm in length and 3 mm in breadth, with a straight tail end [Fig. 3] and [Fig. 4]. The presence of a vulvar waist confirmed it as a female adult worm of A. lumbricoides.
Fig. 2: Chocolate brown-coloured frank pus drained from the liver abscess
Fig. 3: Macerated parasite which emerged through a pigtail catheter
Stool examination did not reveal eggs of A. lumbricoides or Charcot-Leyden crystals. The patient was treated with albendazole, corticosteroids, and metronidazole washes administered via the pigtail catheter. Subsequently, the patient became drowsy, initially arousable but later disoriented. Air entry was decreased bilaterally, and creatinine levels increased. She was transferred to the intensive care unit and eventually succumbed to sepsis with acute respiratory distress syndrome and multiple organ dysfunction.
DISCUSSION
Human helminthiases rank among the most widespread parasitic infections globally, with A. lumbricoides being the most prevalent species implicated. Its high prevalence correlates with regions characterised by poverty, substandard housing, overcrowding, and inadequate environmental sanitation [5, 6].
The infective stage for humans is the fully embryonated egg containing a larva. Upon ingestion, these eggs hatch in the small intestine, releasing motile larvae. The larvae penetrate the intestinal mucosa and enter the portal circulation, thereby reaching the liver. After a sojourn of 3 to 4 days in the hepatic tissue, the larvae migrate via the systemic circulation to the lungs. There, they undergo further development over 10 to 15 days, eventually penetrating the pulmonary capillaries to enter the alveoli. Subsequently, the larvae ascend the bronchial tree, passing through the trachea, larynx, and pharynx, before being swallowed over the epiglottis with saliva. In the intestine, the worms mature within 6 to 10 weeks, mate, and produce eggs, which are excreted in the stool [7]. Notably, a minimum of 65 days is required post-infection before eggs can be detected in stool samples [3]; this observation may account for the absence of eggs in the stool in the present case.
The adult worm primarily inhabits the gastrointestinal tract and is often asymptomatic. However, adverse intestinal conditions—such as inflammation or obstruction—may prompt the migration of Ascaris worms to extraintestinal sites. Such aberrant migration can result in severe intra-abdominal complications, significant malnutrition, increased morbidity, and even mortality [8]. Hepatic abscess attributable to A. lumbricoides lacks pathognomonic clinical features that distinguish it from liver abscesses of other aetiologies [9].
Chauhan V et al. (2015) described three cases from Himachal Pradesh: in the first, a pigtail catheter inserted to drain a hepatic abscess yielded a coiled worm in the drainage bag, later identified as Ascaris. The second case involved a patient who vomited an Ascaris worm, and the third case also noted a coiled worm in the pus collection bag, suggestive of ascariasis [10]. These presentations closely resemble our case report. The worms retrieved from the drainage bag are typically macerated, facilitating their passage through the small bore of the pigtail catheter [10].
According to Javid G et al., among 510 cases of liver abscess evaluated over a decade in Kashmir (December 1987 to December 1997), 74 involved biliary ascariasis. Of these, 11 patients had intact ascarids (either live or dead) within the abscess. Six patients had solitary abscesses, while five had multiple abscesses. Ultrasonography served as the principal diagnostic modality, with 10 cases diagnosed by clinical assessment and imaging, and one case identified during laparotomy[11].
Peripheral eosinophilia represents a host immune response to parasitic infection and is more pronounced during larval migration or when eggs are deposited within hepatic tissue, as observed by Analida E et al., who reported an eosinophil count of 17%[4]. In the current case, there was no marked eosinophilia; however, anaemia and mild leucocytosis with neutrophilia were evident. No significant co-morbidities were documented, except for the patient’s advanced age, which may have adversely influenced the prognosis.
Hepatic abscess secondary to Ascaris lumbricoides remains an exceedingly rare complication but can progress to multi-organ failure and death[12]. It is imperative that all cases of liver abscess be evaluated for possible ascariasis[10].
CONCLUSION
This case report underscores the importance of heightened clinical awareness. Early recognition of clinical features, timely diagnosis, and appropriate treatment are essential for reducing mortality and morbidity associated with this condition.
References
Pinilla AE, Lopez MC, Ricaurte O, Toledo B, Murcia M, Nicholls RS, <I>et al</I>
Liver abscess caused by <I>Ascaris lumbricoides</I>: case reportRevista do Instituto de Medicina Tropical de São Paulo2001436https://doi.org/10.1590/s0036-46652001000600010
Castro MB
Ascariasis: complicaciones hepatobiliares, Hospital Universitario San José, Popayán, 1984-1993Colombia Medica1995262https://doi.org/10.25100/cm.v26i.2.1743
Fogaca HS, Oliveira CS, Barbosa HT, Lanfredi RM, Chagas V
Liver pseudotumor: a rare manifestation of hepatic granulomata caused by <I>Ascaris lumbricoides</I> ovaThe American Journal of Gastroenterology2000958https://doi.org/10.1111/j.1572-0241.2000.02276.x
Chauhan V, Thakur S, Rana B
Ascariasis as a cause of hepatic abscess: A report of 3 casesIndian Journal of Medical Microbiology2015333https://doi.org/10.4103/0255-0857.158576
Javid G, Wani NA, Gulzar GM, Khan BA, Shah AH, Shah OJ, <I>et al</I>
<i>Ascaris</i>‐induced Liver AbscessWorld Journal of Surgery19992311https://doi.org/10.1007/s002689900645
Medina Andrade L, Aguilar L, Duarte E, Rodriguez C, Mendoza A
Liver Abscess Secondary to <I>Ascaris lumbricoides</I>: Case ReportArchives of Clinical Gastroenterology201623https://doi.org/10.17352/2455-2283.000027