Volume: 14 Issue: 1
Cervical Lesions among HIV-Positive Women receiving Highly Active Antiretroviral Therapy in Jos, Nigeria
Year: 2026, Page: 29-36, Doi: https://doi.org/10.47799/pimr.1401.25.74
Received: Oct. 21, 2025 Accepted: April 3, 2026 Published: May 1, 2026
Abstract
Introduction: Cervical lesions and HIV are significant public health concerns, particularly in sub-Saharan Africa, where women face a disproportionate burden of both conditions. Despite advancements in Highly Active Antiretroviral Therapy (HAART), the relationship between HAART and cervical lesion progression remains unclear, especially in resource-limited settings. Aim and Objectives: This study aimed to investigate the prevalence and characteristics of cervical lesions among HIV-positive women on HAART. Materials and Method: A cross-sectional design was used, recruiting 351 HIV-positive women from the APIN clinic and 162 HIV-negative women from the gynecological clinic at Jos University Teaching Hospital, Nigeria. Smears were collected, stained using Papanicolaou staining method, and examined for premalignant lesions. Result: Our data revealed a 16.1% prevalence of cervical lesions among HIV-positive women on HAART, with no significant difference compared to those not on HAART (6.2%, p=0.484). However, women on second and third-line HAART exhibited higher lesion severity (23.1% ASC-US, 7.7% ASC-H) compared to those on first-line therapy (88.2% negative results, p=0.044). Behavioral factors, such as multiple sexual partners, were significantly associated with lesion prevalence (p=0.013). Awareness of cervical screening was high (93.7%), but utilization did not significantly reduce lesion prevalence. Conclusion: The findings underscore the complex interplay between HIV, HAART, and cervical lesions, highlighting the need for integrated care models that combine HIV management with regular cervical screening.
Keywords: Cervical lesions, Histopathology, Human Immunodeficiency Virus
BACKGROUND
The well-being of women, particularly those living with Human Immunodeficiency Virus (HIV), is challenged by numerous health conditions[1]. Worldwide an estimate of 20.1 million women is known to be living with HIV[2], and the situation is not different in Nigeria, with an estimated 2 million individuals living with the virus[3]. HIV is a direct threat to the immune system and also carries with it associated health concerns, exposing women to various vulnerable complications. One such is the heightened susceptibility of HIV-positive women to cervical lesions[4]. The link between HIV infection and the elevated risk of developing cervical lesions among women have been sighted in several studies[5, 6]. The interplay of HIV and cervical health highlights the need to explore into this intricate relationship, understanding its implications for comprehensive healthcare. Cervical lesions compromise the reproductive health of women and also serve as potential precursors to more severe conditions, including precancerous and cancerous conditions[7, 8].
Furthermore, there is a great deal of curiosity in how HAART can affect cervical health. It is critical to look into the potential influence of HAART on the onset or development of lesions given the intricate connections that appear to exist between HIV infection and cervical lesions. Research suggests that the immune-suppressive effects of antiretroviral medication might influence the health of the cervical region[9].
Buoyed by rising global optimism about the possibility of reducing cervical cancer globally, the World Health Organization (WHO), with endorsement from over 194 countries, including Nigeria, has recently launched a global initiative to accelerate the elimination of cervical cancer as a public health problem by significant expansion of efforts to increase HPV vaccination to 90% coverage, screening to 70% coverage in mid-adult women, and treatment to 90% of those in need of it[10, 11].
MATERIAL AND METHOD
Study Design
The study was a cross-sectional descriptive study that was conducted two clinics, the cytology section of the Reproductive Health Unit (RHU) of the Aids Preventive Initiative of Nigeria (APIN), for HIV-positive women who were attending the adult HIV clinic and the Obstetrics and Gynaecology clinics for non-HIV infected women in Jos University Teaching Hospital (JUTH), Jos, between April, 2024 to September 2024.
Study Area
The study was carried out at the Reproductive Health Unit (RHU) of the APIN/Harvard PEPFAR HIV Clinic, Jos University Teaching Hospital (JUTH), Nigeria (Appendix A1).
Study Population
The targeted study populations were consenting HIV-positive women recruited in AIDS Prevention in Nigeria (APIN) adult outpatient clinic and those that visited for routine follow-up and drug top-ups.
Inclusion
The followings women were included who consent to participate in the study-
-
HIV-positive women aged 18 years and above.
-
Non-pregnant women and those who were 6 weeks post-partum.
-
HIV-positive women on HAART and not yet on HAART.
-
HIV-negative women.
Exclusion
The followings were excluded to participate in the study-
-
Women who do not give consent to participate in the study.
-
Puerperal (virgin), or menstruating
-
Pregnant women.
-
Women with previous treatment for cervical premalignant lesions, hysterectomy or invasive cervical malignancy
Sample Size
The Fischer ‘s formula below will be used to calculate sample size of the participants that will participate in this study[13]
The sample size was determined using the formula, where Zα is 1.96 at a 95% level of confidence, P is 0.12 a prevalence of 12.3%, d is the 0.05 margin of error, and N is the samples.
Where:
-
N = sample size
-
Zα = normal deviation at the desired confidence interval. In this case it will be taken at 95%, Z value at 95% is 1.96.
-
At significant level of 0.05 and 95% confidence level for a descriptive study, Z α =1.96
-
P = 12.3% prevalence of cervical lesions in HIV positive women[14].
-
= (12/100=0.12)
-
d = degree of precision 5% for this study = (5/100=0.05)
A total of 5 different groups will be used in this study,
Post- HAART which consists of 3 sub-groups
-
first-line regimen group
-
second-line regimen group
-
third-line regimen group
Pre- HAART (naïve) which serve as
-
Comparison group
HIV-Negative, which will serve as
-
Negative control
The sample size was determined using Fischer's formula, yielding 162 participants per group (Total 810). To account for an anticipated attrition rate of 20%, the sample size per group was increased to 200, resulting in a total target population of 1,000 (5 groups × 200).
Ethical Clearance
A letter of introduction with reference number UJ/EC/APIN/FHST/MLS/09, was obtained from the Department of Medical Laboratory Science Faculty of Health Sciences and Technology, College of Health Science, University of Jos. The protocol for this study was approved by the Jos University Teaching Hospital Health Research Ethics Committee with reference number REF/JUTH/DCS/REC/127/XXXI/2664. Permission was obtained from the Harvard School of Public Health for both the identification and enrollment of HIV-infected women in JUTH APIN clinic and the use of secondary data and other relevant information needed for this study.
Data Collection
Cytology specimen
The smears were allowed to fix in the fixative (95% ethanol) for at least 30min, the fixed slides were then rinsed in 2 changes of water for 2min each, slides were stained in Harris haematoxylin for about 4 min and rinsed in 2 changes of water for 2 min. The smear was decolorized with 0.1% acid alcohol briefly and processed using standard techniques as described[15, 16].
Data Analysis
Data obtained were entered into Microsoft Excel worksheet and exported to SPSS software. The data were analyzed by descriptive statistics such as frequencies and percentages using the Statistical Package for Social Science (SPSS) version 26. The association between cervical lesions and HAART was assessed using statistical methods like chi-square tests, and Fisher’s exact the prevalence and severity of cervical lesions among HIV-women on HAART and HAART-naïve HIV- positive women was determined, statistically significant was tested at 5% level of significant (95% C.I) when p-value<0.05.
RESULTS
A total number of 351 HIV positive-women were recruited from the out-patients APIN clinic and 162 HIV-negative women from the gynecological clinic all within Jos University Teaching Hospital, Jos. The participants were separated into five groups: Post-HAART group (which consists of first-line regimen group, second-line regimen group, and third-line regimen group), Pre-HAART or naïve group, which serves as the comparison control group (HIV-positive but not on HAART), and HIV-negative group which serves as the negative control. A structural questionnaire was administered to all respondents. The majority of participants on HAART were middle-aged. Specifically, 36 participants (7.0%) were aged 30 years and below, 95 (18.5%) were between 31 and 40 years, 203 (39.6%) were between 41 and 50 years, and 133 (25.9%) were between 51 and 60 years. Regarding marital status, 46 participants (9.0%) were single, 18 (3.5%) were separated, and 12 (2.3%) were divorced. In terms of educational attainment, 20 participants (4.0%) had no formal education, 104 (20.8%) attained only primary education, 158 (31.5%) had completed secondary education, while 219 (43.7%) had attained tertiary-level education. The highest prevalence of cervical lesions was found in the age group 41-50 years (39.6%) across all groups. Participants were predominantly married (60.0%) and had a secondary or tertiary level of education (75.2% combined). Occupational-wise, business constituted the largest group (38.6%), followed by civil servants (32.2%) [Table. 1].
Women who had previously undergone cervical screening demonstrated a marginally higher prevalence of cervical lesions (18.3%) compared to those who had never been screened (12.0%); however, this difference also did not reach statistical significance (p = 0.130) [Table. 2].
Notably, women with multiple life partners had a lower prevalence of cervical lesions (11.9%) than those with a single spouse (22.0%), with a statistically significant association (p = 0.013). The use of contraceptives, alcohol intake and smoking did not significantly affect the prevalence of cervical lesion in this study (p>0.05) [Table. 3].
HIV-infected women on HAART had a prevalence of 16.12% of cervical lesion when compared with those HIV-infected that are HAART naïve (6.22%) [Table. 4].
Participants on the first line of HAART had the highest proportion of negative results (88.2%) and low prevalence of cervical lesions (11.8%). Whereas, the third-line therapy groups had a lower proportion of negative results (61.5%) and a higher prevalence of lesions, especially ASC-US (23.1%) and LSIL and HSIL had 7.7% each [Table. 5].
|
Demographics |
Groups |
|||
|---|---|---|---|---|
| On HAART n(%) | Comparison group n(%) | Negative control n(%) | Total n(%) | |
| Age groups (yrs) | ||||
| ≤30 | 15(4.5) | 3(18.8) | 18(11.1) | 36(7.0) |
| 31-40 | 52(15.5) | 10(62.5) | 33(20.4) | 95(18.5) |
| 41-50 | 148(44.2) | 2(12.5) | 53(32.7) | 203(39.6) |
| 51-60 | 92(27.5) | 1(6.3) | 40(24.7) | 133(25.9) |
| 61-70 | 28(8.4) | 0(0.0) | 18(11.1) | 46(9.0) |
| Marital status | ||||
| Married | 164(49.0) | 8(50.0) | 136(84.0) | 308(60.0) |
| Single | 24(7.2) | 6(37.5) | 16(9.9) | 46(9.0) |
| Widowed | 120(35.8) | 1(6.3) | 8(4.9) | 129(25.1) |
| Divorced/Separated | 27(8.1) | 1(6.3) | 2(1.2) | 30(5.8) |
| Level of education | ||||
| Non-formal | 20(6.0) | 0(0.0) | 0(0.0) | 20(4.0) |
| Primary | 86(26.0) | 1(7.1) | 17(10.9) | 104(20.8) |
| Secondary | 116(35.0) | 5(35.7) | 37(23.7) | 158(31.5) |
| Tertiary | 109(32.9) | 8(57.1) | 102(65.4) | 219(43.7) |
| Occupation | ||||
| Civil servant | 89(26.6) | 4(25.0) | 72(44.4) | 165(32.2) |
| Business | 241 (71.9) | 8(50.0) | 70(43.2) | 334(65.1) |
| Student | 5(1.5) | 4(25.0) | 5(3.1) | 14(2.7) |
Table 1: Demographic characteristics of participants
| Variables (n=335) |
Cervical lesions |
X2 | p-value | |
|---|---|---|---|---|
| Positive n(%) | Negative n(%) | |||
| Awareness of cervical screening | ||||
| Yes | 52(16.6) | 262(83.4) | 0.721 | 0.396 |
| No | 2(9.5) | 19(90.5) | ||
| Screened | ||||
| Yes | 40(18.3) | 178(81.7) | 2.292 | 0.130 |
| No | 14(12.0) | 103(88.0) | ||
Table 2: Awareness and Distribution of cervical lesions
Significant value P < 0.05
| Risk factors |
Cervical lesions |
X2 | p-value | |
|---|---|---|---|---|
| Positive n(%) | Negative n(%) | |||
| Contraceptive use | ||||
| Yes | 29(14.3) | 174(85.7) | 1.281 | 0.258 |
| No | 25(18.9) | 107(81.1) | ||
| No of life partners | ||||
| Single | 31(22.0) | 110(78.0) | 6.197 | 0.013 |
| Multi life partners | 23(11.9) | 171(88.1) | ||
| Alcohol intake | ||||
| Yes | 11(12.1) | 80(87.9) | 1.502 | 0.220 |
| No | 43(17.6) | 201(82.4) | ||
| Ever smoked cigarette | ||||
| Yes | 2(33.3) | 4(66.7) | 1.339 | 0.247 |
| No | 52(15.8) | 277(84.2) | ||
| Type of marriage | ||||
| Monogamous | 42(16.7) | 209(83.3) | 0.004 | 0.949 |
| Polygamous | 10(16.4) | 51(83.6) | ||
Table 3: Behavioral risk factors and Prevalence of cervical lesions
Significant value P< 0.05
| Cervical lesions |
Group |
X2 | p-value | |
|---|---|---|---|---|
| Post-HAART (%) | Pre-HAART (%) | |||
| Positive | 54(16.1) | 1(6.2) | - | 0.484f |
| Negative | 281(83.9) | 15(93.8) | ||
Table 4: Prevalence of cervical lesions in HIV positive women
fFisher’s exact test→ used When one or more cells in a 2x2 contingency table has an expected frequency of <5. Significant value P< 0.05
| Stages of cervical lesions |
Lines of therapy |
X2 | p-value | ||
|---|---|---|---|---|---|
| First line n(%) | Second line n(%) | Third line n(%) | |||
| Negative | 142(88.2) | 131(81.4) | 8(61.5) | 15.875 | 0.044 |
| ASC-US | 12(7.4) | 15(9.3) | 3(23.1) | ||
| LSIL | 3(1.9) | 7(4.3) | 1(7.7) | ||
| HSIL | 4(2.5) | 8(5.0) | 1(7.7) | ||
Table 5: Association between stages of cervical lesions and HAART’s therapy
Significant value P< 0.05
Key
ASC-US - Atypical squamous cells of -undetermined significance
LSIL - low-grade squamous intraepithelial lesion
HSIL - high-grade squamous intraepithelial lesion
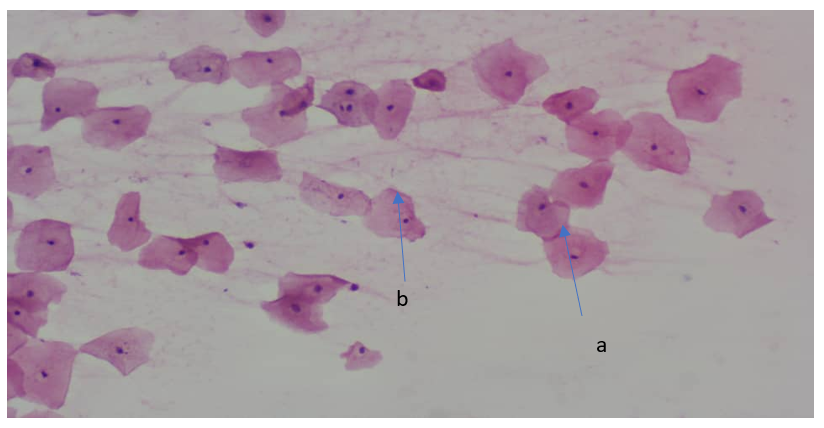
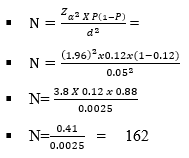
Fig. 1: Cervical smear showing Negative for Intraepithelial Lesion, with pink-stained cytoplasm having well define boards, abundant cytoplasm & low nuclear/cytoplasmic ratio. (a), condensed pyknotic nucleoli, centrally located (b) (Pap Smear; Mag x 40)
Fig. 2: x40 (Papanicolaou stain) cervical smear showing Atypical Squamous Cells of-Undetermined Significance (ASC-US), with hyperchromatic crowed groups of small parabasal cells (a), with slightly enlarged darker nuclei with nucleoli with irregular contours (b & c). (Pap Smear; Mag x 40)
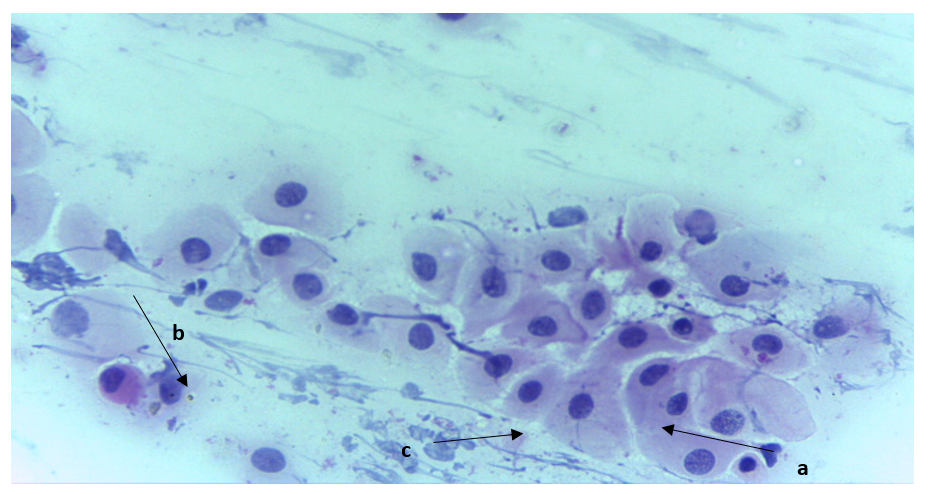
Fig. 3: x40 (Papanicolaou stain) cervical smear showing Low-grade Squamous Intraepithelial Lesion (LSIL), with nuclear being enlarged, coarse but evenly distributed chromatin pattern, hyperchromasia and irregular nuclear contour (a), there is an abundant delicate cytoplasm (b) with presence of koilocytes (c) (Pap Smear; Mag x 40)
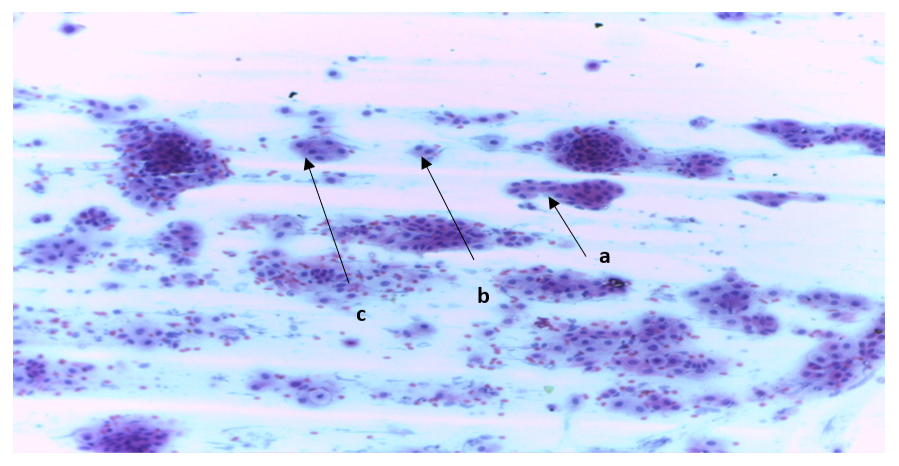
Fig. 4: x40 (Papanicolaou stain) High-grade Squamous Intraepithelial Lesion (HSIL). Cervical smear showing nuclear with hyperchromatic crowded group of cells without distinct cells border (a). very high nuclear cytoplasmic ratio (b & c)
DISCUSSION
Cervical lesions especially Cervical cancer is a leading cause of cancer-related mortality among women globally, with human papillomavirus (HPV) infection playing a pivotal role in its pathogenesis[15, 17]. HIV-positive women are disproportionately affected due to immune suppression, which accelerates HPV persistence and progression to cervical lesions[18]. The advent of Highly Active Antiretroviral Therapy (HAART) has significantly improved the prognosis of HIV infection; however, its role in mitigating cervical lesions remains an area of ongoing research[19, 20].
The present study also observed that the majority of participants across all groups fall within the 41-50 years age group (39.6%). Among those on HAART, 44.2% are aged 41-50 years, followed by those aged 51-60 years (27.5%), suggesting that middle-aged women form the bulk of our population. These findings align with previous reports[21] in Lagos, and in Benin City[22], and recent research in Nigeria, which observed that the peak prevalence of HIV infection occurs among individuals aged 30-50 years[23]. These studies reported a high prevalence of cervical lesions[24-26]among middle-aged women. Similar observation was reported[27], a higher prevalence of cervical lesion among women aged 40-49 years in Cameroon. In Abuja, Ononogbu[28] observed the risk for cervical premalignant and cancer to be associated with age ≤ 40 years. Married participants make up to 60% of the population which emerged as a significant demographic factor, reflecting previous reports[29, 30] which suggested that marital status influences health-seeking behavior. While widowed individuals are significantly represented at 25.1%, particularly in the HAART group (35.8%), this is consistent with studies that associate spousal loss with HIV-related mortality and increased risk of HIV acquisition among widowed women[31].
Our data further showed that 83.4% of women who were aware of cervical cancer screening did not have cervical lesions, compared to 90.5% among those unaware of cervical cancer screening (p = 0.396). Although, this showed that awareness alone is not significantly associated with cervical lesion prevalence in this study, which is consistent with previous reports[32, 33]. Interestingly, a comparison of the prevalence of cervical lesions among HIV-positive women and HIV-negative women, revealed a significantly higher prevalence among HIV-negative women (29.6%, p = 0.001). This contrasts with studies from Ethiopia and Kenya, where cervical lesion prevalence was higher in HIV-positive women[34]. And so many other studies in Nigeria[35-37]. The lower prevalence in this study may be due to HAART's protective effect in reducing HPV persistence and cervical lesion progression[38] or disparities in cervical screening practices among HIV-negative populations[39]. However, ongoing screening is necessary, as HIV remains a major risk factor for persistent HPV infection[26, 40, 41]. Nonetheless, this study has some limitations, and the results should be interpreted with care. We conceived recruitment challenges. There was difficulty enrolling participants due to strict eligibility criteria, lack of interest, and limited access to the target population. We also speculate some reporting bias in the questionnaires administered to the participants. Furthermore, participants withdrawing from the study, leading to a reduced sample size.
CONCLUSION
The findings of this study provide valuable insights into the prevalence of cervical lesions among HIV-positive women, and associated risk factors on cervical health in the study area. While awareness and previous screening did not show significant protective effects, the persistence of cervical lesions underscores gaps in preventive practices. This study highlights the importance of strengthening cervical cancer screening programs, promoting adherence to HAART, and integrating HPV vaccination and lifestyle interventions to reduce the burden of cervical lesions among HIV-positive women.
DISCLOSURE
Acknowledgement: The protocol for this study was approved by the Jos University Teaching Hospital, Health Research Ethics Committee with reference number REF/JUTH/DCS/REC/127/XXXI/2664. Consent was obtained from the Harvard School of Public Health for both the identification and enrollment of HIV-infected women in JUTH APIN clinic and the use of secondary data and other relevant information in the study.
Funding: Nil.
Conflict of Interest: None.
References
1. UNAIDS Data 2020. Joint United Nations Programme on HIV/AIDS.
2. Xiangrong Gao, Gao X, Zhang W, Sun J, Adeloye D, Jin H, Rudan I, et alZhang, Jingyi Sun, Davies Adeloye, Huyi Jin, Igor Rudan, Peige Song, Mingjuan Jin. Lifetime Prevalence and Adherence Rate of Cervical Cancer Screening Among Women Living with HIV: A Systematic Review and Meta-Analysis. Journal of the International Acquired Immunodeficiency Syndrome Society. 2023; 26 (5). Available from: https://doi.org/10.2139/ssrn.4105600
3. Onovo AA, Adeyemi A, Onime D, Kalnoky M, Kagniniwa B, Dessie M, et al. Estimation of HIV prevalence and burden in Nigeria: a bayesian predictive modelling study. E Clinical Medicine, 2023; 62.
4. Gamde SM, Ogunkoya O, Jacob C, Kabir H, Jacob JO, Alhaji U. Knowledge of Cervical Cancer and Vaccine among sexually active Women in FMC, Keffi Nigeria. Research in Medical & Engineering Sciences, 2025:12(1): 000780.
5. Gbinosa II, Ngozi CM, Mathias I, Gamde SM. Prevalence of Cervical Cancer among Sexually Active Women Receiving Antiretroviral Therapy at First Referral Hospital, Mutum Biyu, Nigeria. East African Scholars Journal of Medical Sciences. 2026; 9 (02). Available from: https://doi.org/10.36349/easms.2026.v09i02.007
6. Stumbar SE, Stevens M, Feld Z. Cervical Cancer and Its Precursors. Primary Care: Clinics in Office Practice. 2019; 46 (1). Available from: https://doi.org/10.1016/j.pop.2018.10.011
7. Franzese O, Barbaccia ML, Bonmassar E, Graziani G. Beneficial and Detrimental Effects of Antiretroviral Therapy on HIV-Associated Immunosenescence. Chemotherapy. 2018; 63 (2). Available from: https://doi.org/10.1159/000487534
8. Portilla-Tamarit J, Reus S, Portilla I, Fuster Ruiz-de-Apodaca MJ, Portilla J. Impact of Advanced HIV Disease on Quality of Life and Mortality in the Era of Combined Antiretroviral Treatment. Journal of Clinical Medicine. 2021; 10 (4). Available from: https://doi.org/10.3390/jcm10040716
9. Menon S, Rossi R, Zdraveska N, Kariisa M, Acharya SD, Broeck DV, et al. Associations between highly active antiretroviral therapy and the presence of HPV, premalignant and malignant cervical lesions in sub-Saharan Africa, a systematic review: current evidence and directions for future research. BMJ Open. 2017; 7 (8). Available from: https://doi.org/10.1136/bmjopen-2016-015123
10. Das M. WHO launches strategy to accelerate elimination of cervical cancer. The Lancet Oncology. 2021; 22 (1). Available from: https://doi.org/10.1016/s1470-2045(20)30729-4
11. Selji Y, Adisa JO, Gamde SM, Bali KI, Udo MS, Ikeh CA. Knowledge and Risk Factors of Intraepithelial Lesion amongst Women of Childbearing Age in Jos, Nigeria. Journal of Applied Sciences & Environmental Management. 2025; 29 (4): 1141-1147
12. Peter AS, Matthias GS, Ezekiel C, Benedo OH. Evaluation of Some Liver Enzymes in HIV/AIDS Patients on Antiretroviral Therapy in University of Abuja Teaching Hospital, Nigeria. International Journal of Human and Health Sciences (IJHHS). 2024; 8 (2). Available from: https://doi.org/10.31344/ijhhs.v8i2.632
13. Araoye MO. (2003). Research methodology with statistics for health and social sciences. Ilorin: Nathadex Publishers.
14. Okunade KS. Human papillomavirus and cervical cancer. Journal of Obstetrics and Gynaecology. 2020; 40 (5). Available from: https://doi.org/10.1080/01443615.2019.1634030
15. Gamde MS, Adeleye TM, Adisa JO. Review on Histopathological Techniques in Cervical Cancer Screening. Asian Pacific Journal of Cancer Care. 2024; 9 (4). Available from: https://doi.org/10.31557/apjcc.2024.9.4.785-791
16. Canadian Cancer Society. (2018). Cervical cancer screening. https://www.cancer.ca/en/cancer-information/cancer-type/cervical/screening/?region=on
17. Prat J. Pathology of cancers of the female genital tract. International Journal of Gynecology & Obstetrics. 2012; 119 (S2). Available from: https://doi.org/10.1016/s0020-7292(12)60027-7
18. Kelly H, Mayaud P, de Sanjose S. Concomitant Infection of HIV and HPV: What Are the Consequences?. Current Obstetrics and Gynecology Reports. 2015; 4 (4). Available from: https://doi.org/10.1007/s13669-015-0132-0
19. Firnhaber C, Westreich D, Schulze D, Williams S, Siminya M, Michelow P, et al. Highly active antiretroviral therapy and cervical dysplasia in HIV‐positive women in South Africa. Journal of the International AIDS Society. 2012; 15 (2). Available from: https://doi.org/10.7448/ias.15.2.17382
20. Blitz S, Baxter J, Raboud J, Walmsley S, Rachlis A, Smaill F, et al. Evaluation of HIV and Highly Active Antiretroviral Therapy on the Natural History of Human Papillomavirus Infection and Cervical Cytopathologic Findings in HIV-Positive and High-Risk HIV-Negative Women. The Journal of Infectious Diseases. 2013; 208 (3). Available from: https://doi.org/10.1093/infdis/jit181
21. Adeoye OA, Oguntayo AO, Durosinmi-Etti FA, Adewole IF. Cervical cancer screening among HIV-positive women in Lagos, Nigeria. Journal of Obstetrics and Gynaecology, 2017; 38(5): 685-689.
22. Akhiwu OJ, Osaretin JO, Aziken ME, Osemwenkha AP. Prevalence of cervical dysplasia and associated risk factors among women living with HIV in Benin City, Nigeria. African Journal of Reproductive Health, 2020; 24(1): 125-133.
23. Akinwunmi BO, Adewole IF, Olaitan SO. The burden of cervical cancer in HIV-infected women in southern Nigeria. Journal of Cancer Research and Practice, 2020; 8(1): 15-22.
24. Anorlu RI, Igwilo CI, Akanmu AS, Banjo AA, Odunukwe NN, Okany CC, et al. Prevalence of abnormal cervical smears among patients with HIV in Lagos, Nigeria. Prevalence of abnormal cervical smears among patients with HIV in Lagos, Nigeria, 2007; 26(2): 143-147.
25. De Andrade AC, Luz PM, Velasque L, Veloso VG, Moreira RI, Russomano F, et al. Factors Associated with Colposcopy-Histopathology Confirmed Cervical Intraepithelial Neoplasia among HIV-Infected Women from Rio De Janeiro, Brazil. PLoS ONE. 2011; 6 (3). Available from: https://doi.org/10.1371/journal.pone.0018297
26. Swende TZ, Ngwan SD, Swende LT. Prevalence and risk factors for cervical squamous intraepithelial lesions among women infected with HIV-1 in Makurdi, Nigeria. International Journal of Women's Health. 2012; 4 Available from: https://doi.org/10.2147/ijwh.s21205
27. Teame H, Addissie A, Ayele W, Hirpa S, Gebremariam A, Gebreheat G, et al. Factors associated with cervical precancerous lesions among women screened for cervical cancer in Addis Ababa, Ethiopia: A case control study. PLOS ONE. 2018; 13 (1). Available from: https://doi.org/10.1371/journal.pone.0191506
28. Ononogbu U, Almujtaba M, Modibbo F, Lawal I, Offiong R, Olaniyan O, et al. Cervical cancer risk factors among HIV-infected Nigerian women. BMC Public Health. 2013; 13 (1). Available from: https://doi.org/10.1186/1471-2458-13-582
29. Ezechi OC, Pettersson KO, Okolo CA, Ujah IAO, Ostergren PO. The Association between HIV Infection, Antiretroviral Therapy and Cervical Squamous Intraepithelial Lesions in South Western Nigerian Women. PLoS ONE. 2014; 9 (5). Available from: https://doi.org/10.1371/journal.pone.0097150
30. Omowhara OB, Ameh S, Banjo AA. Cervical cancer screening awareness and uptake among under-screened women. The Nigerian Health Journal. 2022; 22(4).
31. Evans W, Philipps A, Guo J, Kim E, Pereira N, Pesta D, et al. Prevalence of HPV-positive findings in cytology and histology samples from the uterine cervix: A systematic review and meta-analysis. British Journal of Cancer, 2022; 126(7): 1082-1094.
32. Gamde SM, Udo S, Ngozi CM, Etim II, Biya A, Garba A, et al. Knowledge of Cervical Cancer among Females in North Central Nigeria. International Journal of Human and Health Sciences (IJHHS). 2024; 8 (3). Available from: https://doi.org/10.31344/ijhhs.v8i3.725
33. Gamde SM, Omotola OS, Avwioro GO, Adisa JO. Examining the Challenges and Strategies for Improving Cervical Cancer Screening in Nigeria. International Journal of Human and Health Sciences (IJHHS). 2024; 8 (1). Available from: https://doi.org/10.31344/ijhhs.v8i1.616
34. Kuehn BM. WHO Launches Global Push to Eliminate Cervical Cancer. JAMA. 2021; 325 (3). Available from: https://doi.org/10.1001/jama.2020.25668
35. Jeremiah GI, Ikimalo JI, Fiebai PO, Athanasius BP. Abnormal cervical cytology among HIV-positive women in Nigeria. International Journal of Gynecology & Obstetrics. 2014; 125 (2). Available from: https://doi.org/10.1016/j.ijgo.2013.10.024
36. Mogtomo ML, Malieugoue LC, Djiepgang C, Wankam M, Moune A, Ngane AN. Incidence of cervical disease associated to HPV in human immunodeficiency infected women under highly active antiretroviral therapy. Infectious Agents and Cancer. 2009; 4 (1). Available from: https://doi.org/10.1186/1750-9378-4-9
37. Mbuya W, Mangclaviraj S, Mhalu F, Mwakagile D, Swai AB, Mhalu F, et al. Prevalence of human papillomavirus genotypes in cervical cancer among Tanzanian women. Infectious Agents and Cancer. 2021;16(1): 31.
38. Gedefaw M, Bekele T, Deressa T, Tsegaye T, Getahun M. Prevalence of cervical lesions among HIV-positive and HIV-negative women in Ethiopia. Journal of Cancer Epidemiology. 2022; 1-9.
39. Getinet M, Gelaw B, Sisay A, Mahmoud EA, Assefa A. Prevalence and predictors of Pap smear cervical epithelial cell abnormality among HIV-positive and negative women attending gynecological examination in cervical cancer screening center at Debre Markos referral hospital, East Gojjam, Northwest Ethiopia. BMC Clinical Pathology. 2015; 15 (1). Available from: https://doi.org/10.1186/s12907-015-0016-2
40. Palefsky JM, Strickler HD, Berry SA, Moscicki AB, Minkoff H, Chung MH, et al. HPV persistence and cervical neoplasia in HIV-positive women. The Lancet Oncology. 2021; 22(3): 325-334.
41. Okeudo C, Ezem BU, Ojiyi EC. Cervical cancer screening in HIV-positive women in Imo State, Nigeria. Tropical Journal of Obstetrics and Gynaecology. 2021; 38(1): 58-63.
Copyright
©2026 (Gye) et al. This is an open-access journal, and articles are distributed under the terms of the Creative Commons Attribution License CC-BY 4.0. (https://creativecommons.org/licenses/by/4.0/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
Cite this article
Gye J, Adisa JO, Ogbe I, Gamde SM, Jantiku J, Obadiah T, Lailai AL, Kasuwa D. Cervical Lesions among HIV-Positive Women receiving Highly Active Antiretroviral Therapy in Jos, Nigeria. Perspectives in Medical Research 2026; 14(1):29-36 DOI: 10.47799/pimr.1401.25.74