Volume: 14 Issue: 1
Evaluating The Role of Platelet Rich Plasma in The Management of Chronic Plantar Fasciitis: A Prospective Observational Study
Year: 2026, Page: 9-14, Doi: https://doi.org/10.47799/pimr.1401.25.66
Received: Oct. 5, 2025 Accepted: Nov. 7, 2025 Published: Dec. 9, 2025
Abstract
Background: The thick fibrous aponeurosis originating from medial calcaneal tuberosity and spanning the plantar aspect of foot is plantar fascia. This structure undergoes chronic degenerative changes resulting in clinical condition called plantar fasciitis (PF). PF is by far the commonest cause of chronic heel pain and is often refractory to conventional treatment modalities. Platelet-rich plasma (PRP) derived from centrifugation of autologous blood has been offered as minimally invasive, regenerative, orthobiologic therapy for chronic PF. Our study aims to evaluate the efficacy, safety and consistency of PRP in management of chronic PF. Method: Fifty patients (n=50) having symptoms of chronic PF for atleast six months and failed conservative therapy were given a single dose of autologous PRP injection locally. Patients were evaluated using Visual Analog score (VAS) and American Orthopedic Foot and Ankle Society (AOFAS) score at pre-injection (T0) and Post-injection six months (T1). These scoring systems asses patients for pain, functionality, alignment and endurance. Results: A statistically significant improvement in both the scoring systems was noted at the end of the study period (p < 0.05). Thus demonstrating the beneficial effects of local autologous PRP infiltration in terms of pain reduction and functional improvements. Conclusion: Single dose PRP injection in chronic PF as an alternate to conventional therapy offers unequivocal, consistent and predictable reduction in pain and improvement in functionality. Our study demonstrates that local PRP injection is an effective and safe therapy for chronic PF.
Keywords: Chronic plantar fasciitis, Platelet rich plasma, Orthobiologics, Regenerative medicine, Plantar aponeurosis, AOFAS
INTRODUCTION
Plantar fasciitis (PF) is caused by chronic inflammatory degenerative process of the plantar aponeurosis. This is a thick fibrous sheet of tissues originating from medial calcaneal tuberosity and traverses the entire length of plantar aspect of foot [1, 2]. PF is an exceedingly common cause of heel pain accounting for 10 to 15 percent of total out-patient load in Orthopaedics clinics [2]. Classically PF is described as “start-up pain” when the patient takes first few steps in morning, felt mostly on the medial side of ankle. Pain is also experienced after getting up from extended periods of rest [2, 3]. Classically pain is acute in onset and does not radiate. Gradual relief in heel pain is noticed as the day passes by [2, 3, 4]. Clinical examination reveals pain on passive dorsiflexion of the first toe and tenderness on the medial calcaneal tuberosity [1-4]. Professions requiring prolonged standing, excessive and unaccustomed weight-bearing, or long distance running causes chronic strain and tensile plantar overload resulting in micro-tears of the plantar aponeurosis followed by chronic degeneration [5, 6]. Additional risk factors causatively related to PF are obesity, pes planus, excessive foot pronation and limb length discrepancy and overtly tight Achilles tendon and intrinsic foot muscles [5, 6, 7]. An exhaustive clinical examination should rule out vascular, neurogenic, infectious, oncologic, and systemic reasons for heel pain [5-7]. MR imaging in cases of PF often shows plantar fascia thicker than 6mm with adjacent aponeurotic tissue degeneration.
Histopathological findings in cases of PF show collagen disintegration, micro tears, fibroblastic hyperplasia, myxoid degeneration, and remarkably an absence of acute inflammation. This demonstrates long-term degenerative process rather than acute inflammatory onset disease. There is complete absence of classical polymorphs-lymphocytes type inflammatory infiltration [8].
Therefore, the term "plantar fasciitis" is a misnomer because the disease process is degenerative in nature rather than inflammatory. Conservative treatment is given initially in all cases of PF to start with [9-11].
To control or reverse the degenerative process, therapy or regimens that initiate healing or restorative response as opposed to countering inflammatory process are required [11-15]. Platelet rich plasma (PRP) is one such regenerative and restorative agent and has emerged as a promising treatment option of PF, it is produced by centrifugation of autologous whole blood and is now classified as an “Orthobiologics” [16]. Orthobiologics are organic substances and synthetic materials that help in the cure of musculoskeletal problems to augment the possibilities of curing bone and soft tissue lesions. They provide conducive environment for initiating restorative process. The fundamental orthobiologics are the following: osseous hollow fillers, extracellular matrix (ECM) substances, platelet-rich plasma (PRP), bone morphogenetic protein-2 (BMP-2), bone marrow aspirate (BMA), bone marrow aspirate concentrate (BMAC), and mesenchymal stem cells (MSCs). The scientific basis for the current utilization of orthobiologics is their potential to alleviate symptoms and to enhance the chances of healing of tissues with little intrinsic healing ability such as cartilage, tendons, ligaments, bone, muscle and meniscus. Our study aims to study the efficacy and safety of autologous PRP infiltration in management of chronic PF.
MATERIAL AND METHODS
Study Design
Our is a prospective observational study carried out in a tertiary care Military hospital in the state of Andhra Pradesh. The study protocol was perused and approved by the Institutional Ethics Committee, No. IEC Kalyani/IEC/2025. The study was carried out in accordance to STROBE guidelines. The participants were explained clearly that PRP injection is a well-accepted treatment modality in PF and that data generated from the study will be published in a reputed journal.
Inclusion criteria: 50 (n=50) patients with symptoms and signs of PF who have received at least 12 weeks of non-invasive treatments including rest, physical therapy, and NSAIDs were included in the study.
Exclusion criteria: patients with old ankle/foot fractures, Charcot foot, local infection, malignancy, malformations, immuno-compromised states and auto-immune diseases were excluded from the study. PRP infiltration was given by one of the two Orthopaedic surgeons. The clinical examination was performed in the standard manner for foot and ankle by an experienced registered physiotherapist available in-house ensuring blind nature of the study, in addition by means of a detailed questionnaire incorporating the scoring systems.
Apparatus
We used the Arthrex ACP double-syringe system for producing the autologous PRP injection. This entire apparatus including the centrifuge machine and accessories were available in-house. The Arthrex ACP double-syringe system is state of the art PRP production device that offers several advantages compared to other such systems.
The distinct advantages of Arthrex ACP double syringe system are:
- Allows for rapid and efficient concentration of platelets and growth factors from autologous blood.
- Unique double syringe system allows for a closed system preparation process resulting in safe handling of blood and complete asepsis.
- It has a quicker processing time compared to conventional systems.
-
WBCs and specifically neutrophils are not concentrated within the Arthrex ACP system. These cells have detrimental effects on healing due to release of reactive free radicals.
Anticoagulant Citrate Dextrose A solution (ACD-A) is a citrate based anticoagulant used for preparing PRP. Blood from the patient is directly collected in the Arthrex ACP double syringe, about 15-20 ml of blood collected slowly over 30-40 seconds to prevent haemolysis. The ACP double syringe is then placed directly in the Horizon 24 Flex-AH centrifuge machine which runs at 1500 revolutions per minute (rpm). The PRP thus formed is directly collected in the syringe which is used for local infiltration [Fig. 1]. Stringent asepsis is practised while giving PRP infiltration [Fig. 2]. After painting and draping the foot-ankle, points of maximum tenderness were marked with sterile marker pen. PRP was infiltrated by pushing the needle upto periosteum depth and withdrawing to plantar aponeurosis level. PRP was infiltrated in a fan-shaped wheel, peppering the area seven to ten times [Fig. 2].
The infiltration site was bandaged with sterile crepe bandage. Cold/ice compresses was recommended and NSAIDS given for post-procedure discomfort. Patients were non-weight bearing for 48 hours, and running or jumping was disallowed for 2 weeks. After three weeks, a gradual return to activities was permitted. Follow-up was conducted at three weeks, three months and six months following the procedure, the outcome was evaluated using the modified American Orthopaedic Foot and Ankle Society (AOFAS) score and visual analog score (VAS).
The AOFAS score system has following components: 1. Pain (40 points): evaluates the severity and frequency of pain. 2. Function (50 points): assesses a patient’s ability to perform daily and recreational activities, climb stairs and uneven terrain. 3. Alignment (10 points): clinician determined assessment of hindfoot alignment and range of motion (RoM). Hence, this score combines subjective information obtained from the patient combined with objective clinical assessment. Patient self-reported pain was objectively assessed by the VAS scale with scores in range from 0 (nil observable pain) to 10 (unbearable or worst pain).
Statistical Analysis
Statistical analysis was performed using Jamovi version 2.6.26. Continuous variables were expressed as means and standard deviations (mean±SD). Changes in outcome measures before and after the intervention were evaluated by the paired t-Test. A p-value less than 0.05 was taken as statistically significant, meaning that intervention had made a significant difference in the outcome. Patient details and scores based on the two scoring systems were tabulated on the excel sheet, both at the beginning (T0) and end of study (T1). All these values were then used to calculate the mean, standard deviation and p-values of the scoring system at T0 and T1.
RESULTS
The study included 50 (n=50) participants, with a mean age of 31.9±7.4 years. 34 (68%) patients were female and remaining 16 (32%) were male. Of these (n=50), 19 (38%) patients had bilateral PF and hence received PRP infiltration in both heels. Even though observations were made at 3 weeks, three months and six months, for the sake of simplicity we have shown T0 as pre-injection scores and T1 as scores at the end of study duration i.e. 6 months. Since, this was an institutional study, there was no loss to follow-up.
The AOFAS score increased from 74.0±3.1 at pre-injection to 92.1±1.9 six months post-injection (p<0.001), reflecting significant improvement in foot-ankle function [Table. 1].
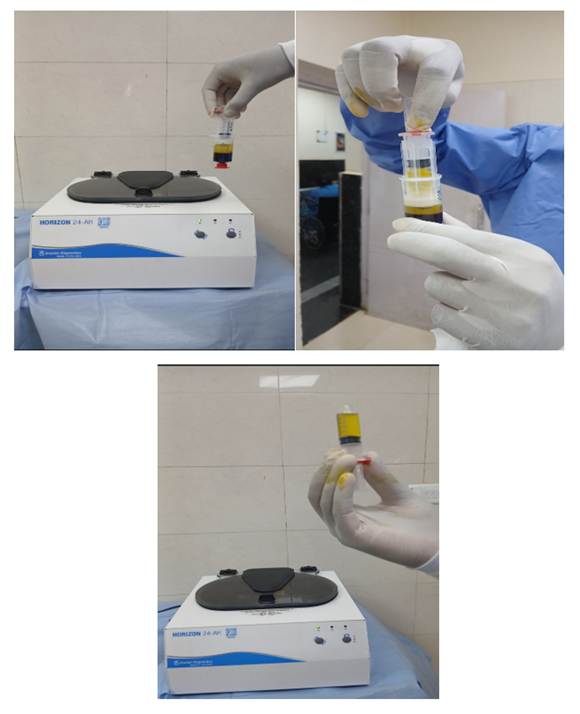
Fig. 1: Preparation of Autologous PRP using the Arthrex ACP double-syringe system

Fig. 2: Under stringent asepsis infiltration of autologous PRP in a fan-shaped wheel, peppering the area five to seven times
This trend was observed in all the three components of AOFAS scores, suggesting improved ambulatory status, physical endurance and mobility [Fig. 3]. Pain levels as assessed by Visual Analog Scale (VAS), reduced from 5.2±1.4 pre-treatment to 2.4±0.8 post-treatment (p<0.001), indicating a clinically meaningful and patient observable reduction in perceived pain in affected ankle [Fig. 4]. [Table. 1] summarises the comparison of Pre and six months Post-PRP infiltration clinical outcomes, enlisting the two scoring systems.
|
Assessment Tool |
Pre |
Post |
Mean |
p-value |
Effect Size |
|---|---|---|---|---|---|
|
AOFAS Score |
74.0 ± 3.1 |
92.1 ± 1.9 |
-8.1 |
<0.001 |
-3.3 |
|
VASScore |
5.2 ± 1.4 |
2.4 ± 0.8 |
2.8 |
<0.001 |
2.4 |
Table 1: Comparison of Pre- and Post-PRP infiltration Clinical Outcomes based on Scoring systems
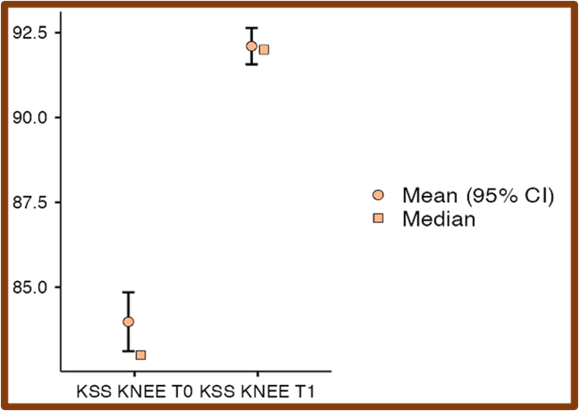
Fig. 3: Comparison of pre- and post-PRP infiltration American Orthopaedic Foot and Ankle Society AOFAS Scores. A notable increase in scores post-treatment indicates significant improvement in ankle-foot function. The plot shows the mean values with 95% confidence intervals (circles with error bars) and medians (squares) for AOFAS scores at baseline (T0) and post-treatment (T1)
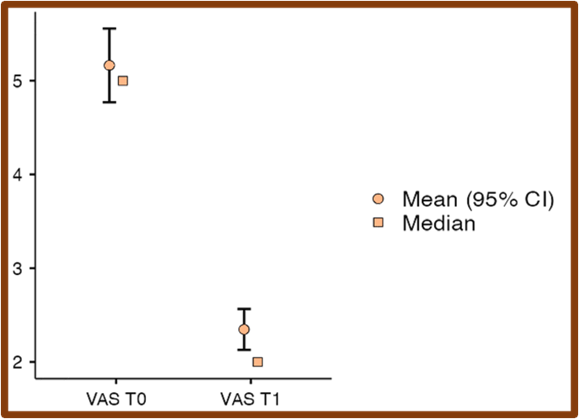
Fig. 4: Comparison of pre- and post-intervention Visual Analog Scale (VAS) pain scores. The significant reduction in VAS scores post-treatment indicates a marked decrease in self-reported pain intensity
DISCUSSION
By far the commonest cause of chronic, unresolving heel pain in Orthopaedics clinics is plantar fasciitis (PF). [1, 2] PF represents chronic degenerative changes in plantar aponeurosis resulting from fibroblastic hyperplasia, collagen disintegration, micro-tears and myxoid degeneration [3, 8]. The aim of our study was to evaluate the short-term outcome, efficacy, safety and consistency of autologous PRP infiltration in the management of chronic PF. Conservative management is given in all cases of PF, this includes rest, NSAIDs, activity modification, cold compresses, deep tissue physiotherapy, acupressure and plantar extension exercises [3, 9, 10, 11, 12]. Plantar extension exercises give most consistent pain relief compared to other conservative modalities [12, 13]. Failure of conservative therapy in PF results in chronicity which adversely affects activities of daily living [2, 3, 4].
Traditionally local corticosteroid infiltration has been the mainstay of treatment of chronic PF [14]. Even though local corticosteroid alleviate heel pain, they inhibit regeneration of fibroblasts and paradoxically accelerate degenerative changes in plantar tissue resulting in heel fat pad atrophy, therefore repeated corticosteroid injections in PF are contraindicated [14, 15].
Amidst the suboptimal results with conservative management and deleterious effects of corticosteroid injection therapy in PF, autologous PRP emerges as a promising option in management of chronic PF [16]. Pathophysiology of PF shows chronic degenerative changes in plantar tissue and complete absence of classical inflammatory polymorph-lymphocyte infiltrate [8]. This is the reason for failure of steroid therapy in PF and a role for regenerative agent. PRP is one such restorative, regenerative agent classified as an Orthobiologic. PRP contains various growth factors like insulin-like growth factor (IGF), transforming growth factor beta (TGF-B), Platelet-derived growth factor (PDGF), cytokines and interleukins. Collagen synthesis, fibroblast proliferation and neo-angiogenesis are promoted by PRP [16].
Kesikburun B, et al in their randomized controlled trial (RCT) compared the effects of injection PRP with placebo. They found that PRP gives significantly better pain control on VAS score compared to placebo [17]. Monto RR, et al. in another RCT compared PRP with local corticosteroid injection [18]. They observed that for upto six months PRP gives better pain control with much lower VAS scores than steroids [18]. Likewise multiple RCTs have compared the results between steroid and PRP, and all of them reported consistently better results for PRP with almost nil adverse effects [17, 18, 19, 20, 21].
Xue Yet al in their systematic review and meta-analysis of RCTs found significant improvement in AOFAS scores with PRP compared to local steroid injections [19]. Kalaci A et al. in their RCT compared the effects of four different injections and found consistently superior results for PRP [22].
The findings in our study also showed that both on pain and functionality scores, PRP gives consistent and predictable results. This was in concurrence with other studies on the role of PRP in PF [23, 24]. VAS scores were significantly lower at six months after the injection compared to pre-injection period in our study. Pre-injection VAS scores on average were 5.2 ± 1.4, in post-injection after six months were 2.4±0.8. This unequivocally showed a significant reduction in patient self-reported pain. The AOFAS average score improved from 74.0±3.1 in pre-injection period to 92.1±1.9 six months after injection. This demonstrated a consistent improvement in pain, functionality, endurance and ability to perform daily and recreational activities.
Our study however had certain limitations also. The authors are aware of the short follow-up of the clinical study. The post-procedure follow-up period was short and therefore it might limit utilisation of the present study in clinical scenario. Hence long term effects follow-up studies ae required to validate the results and be more meaningful in clinical settings. Another limitation of our study was that there was no comparison group like a placebo or steroid group to compare the results of PRP with other treatment modalities.
CONCLUSION
PF is caused by chronic degenerative processes in plantar tissue and therefore a regenerative-restorative approach like PRP gives consistently better results. Our study unequivocally shows PRP as a reliable treatment modality in PF with predictable results. We recommend use of PRP as an effective treatment option for PF, wherever facilities exist and cost permits.
DISCLOSURE
Ethical statement
The protocol and registration of this study was approved by the institutional ethics committee (IEC) of our hospital.
Data and Statistics Availability
The data and statistical analysis presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflict of interest
The authors declare no conflict of interest.
Funding and sponsorship statement
This research received no external funding or financial/material support.
References
1. Schwartz EN, Su J. Plantar Fasciitis: A Concise Review. The Permanente Journal. 2014; 18 (1). Available from: https://doi.org/10.7812/tpp/13-113
2. Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. American Family Physician 2005;72:2237–42.
3. Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a systematic review. Journal of Science and Medicine in Sport. 2006; 9 (1-2). Available from: https://doi.org/10.1016/j.jsams.2006.02.004
4. Johnson RE, Haas K, Lindow K, Shields R. Plantar fasciitis: what is the diagnosis and treatment?. Orthopaedic Nursing. 2014; 33 (4). Available from: https://doi.org/10.1097/nor.0000000000000063
5. Goff JD, Crawford R. Diagnosis and treatment of plantar fasciitis. American Family Physician 2011;84:676–82.
6. Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. British Journal of Sports Medicine. 2002; 36 (2). Available from: https://doi.org/10.1136/bjsm.36.2.95
7. Neufeld SK, Cerrato R. Plantar Fasciitis: Evaluation and Treatment. Journal of the American Academy of Orthopaedic Surgeons. 2008; 16 (6). Available from: https://doi.org/10.5435/00124635-200806000-00006
8. Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. Journal of the American Podiatric Medical Association. 2003; 93 (3). Available from: https://doi.org/10.7547/87507315-93-3-234
9. Podolsky R, Kalichman L. Taping for plantar fasciitis. Journal of Back and Musculoskeletal Rehabilitation. 2015; 28 (1). Available from: https://doi.org/10.3233/bmr-140485
10. Mark Wolgin, Charles Cook, Charles Graham, Don Mauldin. Conservative Treatment of Plantar Heel Pain: Long-Term Follow-Up. Foot & Ankle International. 1994; 15 (3). Available from: https://doi.org/10.1177/107110079401500303
11. Cornwall MW, McPoil TG. Plantar Fasciitis: Etiology and Treatment. Journal of Orthopaedic & Sports Physical Therapy. 1999; 29 (12). Available from: https://doi.org/10.2519/jospt.1999.29.12.756
12. DiGiovanni BF, Nawoczenski DA, Lintal ME, Moore EA, Murray JC, Wilding GE, Baumhauer JF. Conservative treatment of plantar heel pain: long-term follow-up. The Journal of Bone & Joint Surgery. 2003; 85 (7). Available from: https://doi.org/10.2106/00004623-200307000-00013
13. Gupta R, Malhotra A, Masih GD, Khanna T, Kaur H, Gupta P, et al. Comparing the Role of Different Treatment Modalities for Plantar Fasciitis: A Double Blind Randomized Controlled Trial. Indian Journal of Orthopaedics. 2020; 54 (1). Available from: https://doi.org/10.1007/s43465-019-00038-w
14. Acevedo JI, Beskin JL. Complications of Plantar Fascia Rupture Associated with Corticosteroid Injection. Foot & Ankle International. 1998; 19 (2). Available from: https://doi.org/10.1177/107110079801900207
15. Sellman JR. Plantar Fascia Rupture Associated with Corticosteroid Injection. Foot & Ankle International. 1994; 15 (7). Available from: https://doi.org/10.1177/107110079401500706
16. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-Rich Plasma. The American Journal of Sports Medicine. 2009; 37 (11). Available from: https://doi.org/10.1177/0363546509349921
17. Kesikburun B, Tan AK, Yilmaz B, Yaşar E, Yazicioğlu K. Platelet-rich plasma injections in the treatment of chronic plantar fasciitis: a randomized, double-blinded placebo-controlled trial. Journal of the American Podiatric Medical Association. 2018;108:93–100.
18. Monto RR. Platelet-Rich Plasma Efficacy Versus Corticosteroid Injection Treatment for Chronic Severe Plantar Fasciitis. Foot & Ankle International. 2014; 35 (4). Available from: https://doi.org/10.1177/1071100713519778
19. Xue Y, Chen T, Yang Y, et al. Platelet-rich plasma versus corticosteroid injections for plantar fasciitis: A systematic review and meta-analysis of randomized controlled trials. Journal of Orthopaedic Surgery and Research. 2021;16:270.
20. Tekin L, Akarsu S, Durmuş E, et al. Platelet-rich plasma versus corticosteroid injection for plantar fasciitis: a comparative study. Journal of the American Podiatric Medical Association. 2019;109:357–365.
21. Kim E, Lee JH, Park J, et al. Platelet-rich plasma versus steroid injection for plantar fasciitis: a prospective, randomized, single-blinded clinical trial. Regenerative Medicine. 2018;13:743–749.
22. Kalaci A, Çakici H, Hapa O, Yanat AN, Dogramaci Y, Sevinç TT. Treatment of Plantar Fasciitis Using Four Different Local Injection Modalities. Journal of the American Podiatric Medical Association. 2009; 99 (2). Available from: https://doi.org/10.7547/0980108
23. Vahdatpour B, Kianimehr L, Moradi A, Haghighat S. Beneficial effects of platelet-rich plasma on improvement of pain severity and physical disability in patients with plantar fasciitis: A randomized trial. Advanced Biomedical Research. 2016; 5 (1). Available from: https://doi.org/10.4103/2277-9175.192731
24. Martinelli N, Marinozzi A, Carnì S, Trovato U, Bianchi A, Denaro V. Platelet-rich plasma injections for chronic plantar fasciitis. International Orthopaedics. 2013; 37 (5). Available from: https://doi.org/10.1007/s00264-012-1741-0
Copyright
©2026 (Varma) et al. This is an open-access journal, and articles are distributed under the terms of the Creative Commons Attribution License CC-BY 4.0. (https://creativecommons.org/licenses/by/4.0/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
Cite this article
Varma R, Wani S, Zachariah S, Kuriachan D. Evaluating The Role of Platelet Rich Plasma in The Management of Chronic Plantar Fasciitis: A Prospective Observational Study. Perspectives in Medical Research 2026; 14(1):9-14 DOI: 10.47799/pimr.1401.25.66