Volume: 14 Issue: 1
Study of Anomalous Tendons of the Upper and Lower Limb Muscles and their Clinical and Embryological Significance
Year: 2026, Page: 4-8, Doi: https://doi.org/10.47799/pimr.1401.25.62
Received: Oct. 1, 2025 Accepted: Dec. 12, 2025 Published: April 28, 2026
Abstract
Background: Anomalous tendons and accessory muscles of the limbs are uncommon but clinically significant. They may mimic soft-tissue masses or cause compression neuropathies. Awareness of such variations helps in accurate diagnosis and safer surgical interventions. Methods: This cadaveric observational case series was conducted during routine dissections of 120 limbs (upper and lower) over four years. Cadavers with damaged or deformed limbs were excluded. Each specimen was carefully examined for the presence of accessory tendons, and findings were documented photographically. Results: Six unilateral anomalous tendons (5%) were identified. In the upper limb, two cadavers exhibited accessory tendons arising from the extensor carpi radialis longus (ECRL). In the lower limb, one additional tendon arose from the peroneus longus, two from the extensor digitorum longus, and one from the peroneus tertius. All cases were unilateral and showed no associated muscular or skeletal abnormalities. Conclusion: Recognition of anomalous tendons is important for anatomists, radiologists, and surgeons. Such variations may resemble pathological findings on imaging but can serve as valuable grafts in reconstructive and tendon transfer surgeries. Understanding their embryological origin enhances anatomical knowledge and prevents iatrogenic injury during operative procedures.
Keywords: Anomalous tendon, Accessory muscle, Iatrogenic injury, Compression neuropathy, Tendon transfer, Reconstructive surgery
INTRODUCTION
Anomalous tendons of the upper and lower limb muscles carry important clinical relevance. Failure to recognize these variations may lead to misinterpretation in diagnostic imaging, especially ultrasound. A thorough understanding of the architecture and variations of the extensor musculature on the dorsum of the hand is therefore essential for both anatomists and clinicians[1]. Furthermore, knowledge of such traits contributes to the study of human evolutionary development[2]. Rare variants of the extensor carpi radialis muscle must be considered during clinical practice, as they may mimic pathological findings or even contribute to conditions such as radial tunnel syndrome[3].
MATERIAL AND METHODS
Materials
Scalpel, forceps (blunt and toothed) scissors, handheld manual retractors.
Method
During routine cadaveric dissections for 1st-year MBBS students, we observed additional tendons emerging from muscles in both the upper and lower limbs. Cadavers with deformed or severely damaged limbs were excluded from the present study. In the upper limb, two cadavers exhibited an accessory tendon arising from the extensor carpi radialis longus muscle. In the lower limb, one cadaver showed an additional tendon from the peroneus longus muscle, two cadavers had an accessory tendon from the extensor digitorum longus muscle, and one cadaver displayed an extra slip of the peroneus tertius muscle. Altogether, we documented six unilateral cases of accessory tendons.
This case series included 120 dissected limbs over a period of 4 years. Out of these, six cases exhibited anomalous tendons (5% incidence), with unilateral distribution involving both upper and lower limbs. Each variation was photographed and correlated with standard anatomical references.
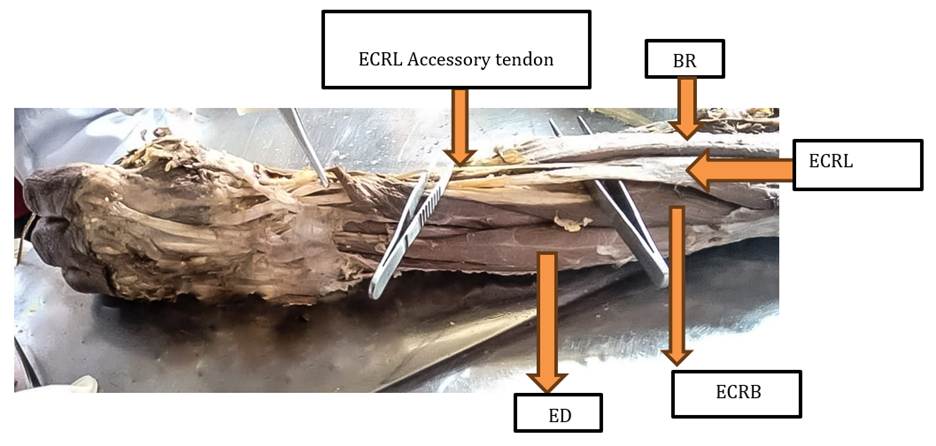
Fig. 1: Photographic representation of the additional extensor carpi radialis longus muscle in the extensor compartment of the forearm in the right upper limb. [ECRL- (Extensor carpi radialis longus muscle); ED- (Extensor digitorum); ECRB- (Extensor carpi radialis brevis); BR- (brachioradialis)]
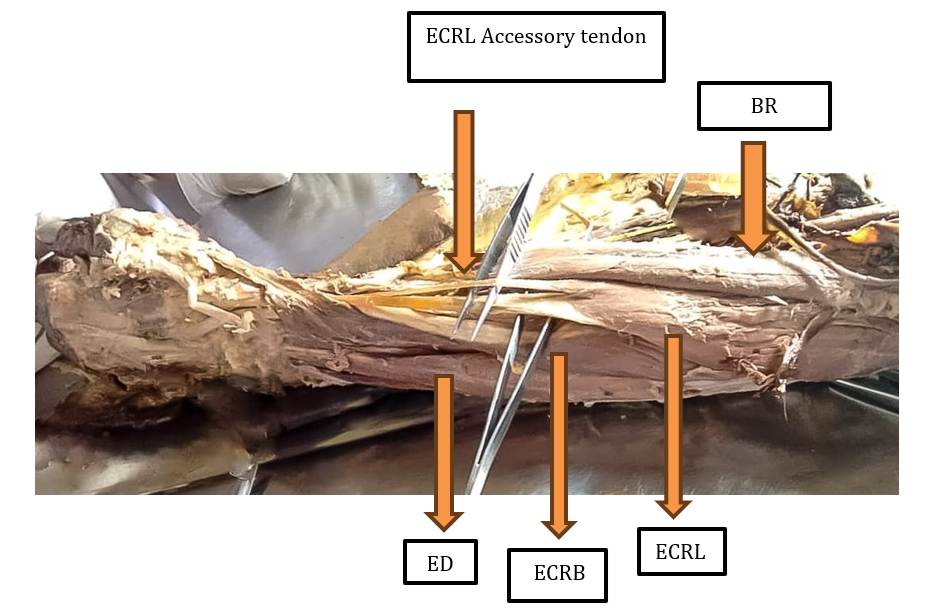
Fig. 2
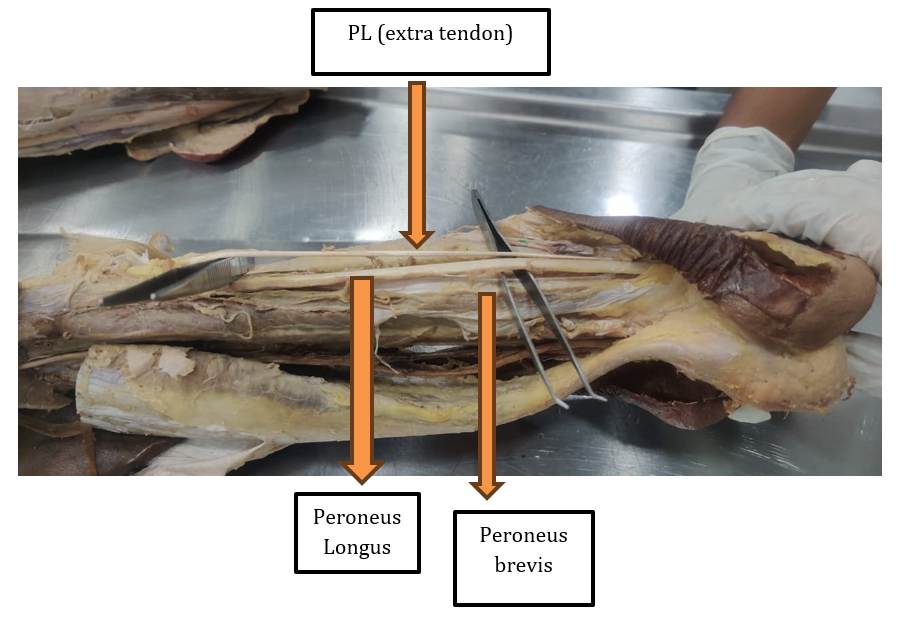
Fig. 3: Photographic representation of extra tendon of PL – Peroneus longus muscle

Fig. 4: Photographic representation of extra tendon of PL – Peroneus longus muscle
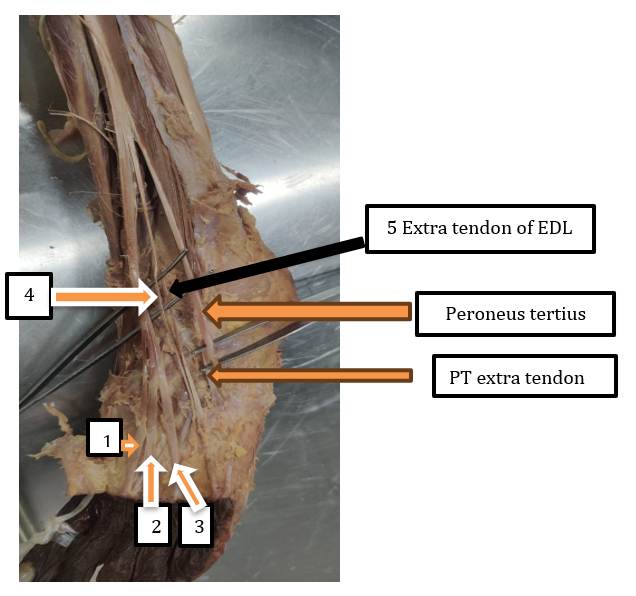
Fig. 5: Photographic representation of EDL- Extensor digitorum longus muscle. 1,2,3,4 EDL tendons and 5 Extra tendon of EDL and PT – Peroneus tertius muscle of the lower limb
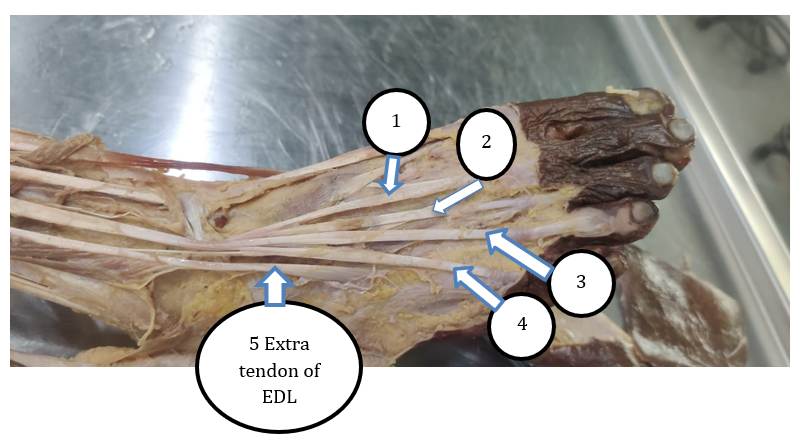
Fig. 6: Photographic representation of EDL- Extensor digitorum longus muscle. 1,2,3,4 EDL tendons and 5 Extra tendon of EDL
DISCUSSION
Several studies have described variations in the extensor compartment of the forearm. For instance, accessory slips have been reported arising from the extensor carpi radialis longus (ECRL)[4]. The combined incidence of ECRL and extensor carpi radialis brevis (ECRB) variations has been reported as approximately 4%[5]. Additional bellies of the ECRL with elongated or flattened tendons have also been documented[6]. Nayak et al. described the extensor carpi radialis tertius (ECRT), which originates from the lateral epicondyle of the humerus and inserts distally into the bases of the second and third metacarpals[7]. Wood et al. reported the presence of the extensor carpi radialis intermedius (ECRI) in nearly 12% of cases, highlighting its potential as a functionally transferable muscle[8].
Other authors have described related variations in forearm musculature, including anconeus epitrochlearis contributing to ulnar neuropathy and cubital tunnel syndrome[9-11], and cases of reversed palmaris longus presenting with pain and paresthesia[12]. A series of patients with dynamic cubital tunnel syndrome linked to anomalous muscles was also documented[13].
From an embryological perspective, limb muscles arise from the paraxial mesoderm and appear as mesenchymal condensations by the seventh week of development[14]. With limb bud elongation, the muscle tissue separates into flexor and extensor groups, which later merge into a common muscle mass. This tissue originates from the lower cervical and upper thoracic myotomes. Under the influence of myogenic regulatory factors, some muscle primordia undergo apoptosis, while persistence of certain fibers may lead to the development of accessory or supernumerary muscles[15-18]. Several authors have reported similar variations in the extensor compartment of the forearm. Rao et al.[15] and Claassen and Wree[14] described comparable accessory slips of ECRL and ECRB, reporting incidences of 3–6%. Nayak et al.[16] documented an additional radial wrist extensor, while Wood[17] identified the extensor carpi radialis intermedius in 12% of cases. These findings support the notion that such variants are not rare and have significant functional implications. Extensor carpi radialis intermedius (ECRI) present in up to 12% of cases (Wood, 1988)[17].
The embryological basis for tendon anomalies arises from deviation in the normal processes of myogenic differentiation, apoptosis, and compartmental separation[2].
Supernumerary tendons of EDL, PL, and PT have been documented in the literature[4].
Accessory slip of ECRL likely represents persistence of a dorsal premuscle segment that normally regresses[14]. Additional slip of EDL may result from incomplete segmentation of the dorsal premuscle mass, leading to duplication of tendon primordia, similar to the patterns described by Rao et al [15]. Extra slip of the pronator teres can be explained by residual fibrous-muscular laminae between the humeral and ulnar heads that fail to undergo programmed remodeling, consistent with embryological interpretations by previous authors[14].
Probable Causes of the presence of anomalous tendons is likely related to embryological persistence of muscle primordia that normally regress during limb differentiation. During myogenesis, the mesenchymal condensations of the limb bud may fail to undergo apoptosis, leading to accessory or supernumerary tendons[14-18] Environmental, genetic, or positional factors influencing muscle patterning and tendon differentiation may also contribute to these anomalies. Thus, the variations in our study can be attributed to minor deviations during partitioning and regression of the limb muscle primordia.
Even recognizing anomalous tendons is crucial for: Surgeons, to avoid iatrogenic injury during orthopedic, reconstructive, or vascular procedures. Radiologists need to correctly interpret ultrasound and MRI findings to prevent misdiagnosis of masses or pathologies.
Reconstructive surgeons may utilize these accessory tendons for a tendon transfer procedure, such as to restore thumb opposition, correct claw hand deformity, or regain dorsiflexion in foot drop.
Anatomists and educators enrich anatomical knowledge and understanding of evolutionary adaptations.
Such tendons may serve as natural grafts for reconstructive surgeries, reducing donor site morbidity[15, 16]. Compression syndromes, accessory tendons in the forearm may modify the space available for neurovascular structures, potentially contributing to entrapment syndromes such as radial tunnel or median nerve compression[7].
In Certain altered tendon mechanics, an additional or aberrant slip may subtly modify the vector of pull, potentially influencing actions such as wrist extension, dorsiflexion of toes, or pronation, depending on the structure involved[17]. Imaging considerations: On MRI or ultrasound, anomalous tendons may mimic soft-tissue masses or appear as pathological splits if unrecognized7. So overall, even when these variations do not produce obvious functional deficits, their recognition is essential for clinicians, radiologists, and surgeons to ensure precise diagnostic interpretation and safe operative planning.
Our finding of a 5% incidence aligns with previously reported ranges of 3–6% for upper limb tendon anomalies[14, 15].
The types of anomalous tendons encountered, particularly those from ECRL, EDL, PT, and PL are consistent with prior reports describing extensor carpi radialis intermedius, extensor carpi radialis tertius, and supernumerary tendons of peroneus muscles[16]. An anomalous tendon may be defined when it meets one or more of the following criteria:
I. Origin arises from an unusual or accessory muscle belly[19].
II. Course deviates from the normal anatomical pathway or presents duplication, bifurcation, or abnormal fusion[14].
III. Insertion occurs at an atypical bony or soft-tissue site[16].
IV. Laterality asymmetry — the variation is unilateral or not mirrored on the contralateral limb[14, 15].
V. Embryological persistence of muscle or tendon primordia that normally regress during development[14].
These criteria collectively help differentiate between normal anatomical variants and clinically significant anomalous tendons. Our findings show Similar frequency, Similar muscles involved (ECRL, EDL, PL, PT) like that of other studies.
Thus, our study supports the concept that such variations, although uncommon, are not rare, and require documentation due to clinical and surgical importance.
This emphasizes that although rare, such tendons are not exceptional and possess definite surgical importance.
Gaps in Current Literature: Although several reports describe individual cases of anomalous tendons, the true incidence and distribution across both limbs remain poorly documented. Most literature focuses on isolated muscle variations rather than comparative, anatomical and embryological correlation. Furthermore, the functional implications and clinical utility of these accessory tendons in reconstructive surgeries have not been adequately evaluated. Very few studies have quantified the percentage occurrence of such anomalies in cadaveric populations, highlighting the need for systematic documentation such as the present study.
CONCLUSION
This study emphasizes the importance of recognizing muscular variations of both the upper and lower limbs and documenting their frequency. Such knowledge not only aids anatomists but is also of practical use to surgeons. In reconstructive surgery, accessory tendons can be valuable in tendon transfer operations, particularly for managing finger clawing and restoring thumb opposition. A functional tendon may be harvested and transferred to replace a damaged or absent tendon. Additional surgical procedures such as tenotomy or tendon lengthening can also be applied to correct contractures. In the lower limb, anomalous tendons may be utilized to restore dorsiflexion or to correct foot deformities associated with neurological disorders. Techniques such as FCR or ECRB tendon transfers, and FDS transfers for adductor plasty demonstrate the diverse clinical applications.
References
1. Dass P, Prabhu L, Pai M, Nayak V, Ganesh K, Janardhanan J. A comprehensive study of the extensor tendons to the medial four digits of the hand. Chang Gung Medical Journal. 2011;34(6):612–9.
2. Diogo R, Matthews LJ, Wood B. A Major Reason to Study Muscle Anatomy: Myology as a Tool for Evolutionary, Developmental, and Systematic Biology. Biological Systems: Open Access. 2012; 01 (01). Available from: https://doi.org/10.4172/2329-6577.1000102
3. Grigoriță L, Gug C, Vaida MA, Jianu AM, Damen NS. An unusual case of unilateral supernumerary extensor carpi radialis muscle. Folia Morphologica. 2019; 78 (4). Available from: https://doi.org/10.5603/fm.a2019.0037
4. Bharambe V, Shevade S, Patel D, Manvikar PR, Bajpayee PG. A study of the extensor tendons of the hand from point of view of evolution. Journal of the Anatomical Society of India. 2017; 66 (2). Available from: https://doi.org/10.1016/j.jasi.2017.12.001
5. Lemon M, Belcher HJ. An Anomalous Flexor Carpi Ulnaris. Journal of Hand Surgery. 2002; 27 (2). Available from: https://doi.org/10.1054/jhsb.2001.0705
6. Alvin M, Alan N, Leone J, Fredieu JR. A unilateral accessory flexor carpi ulnaris muscle observed during cadaveric dissection. Clinical Anatomy. 2011; 24 (8). Available from: https://doi.org/10.1002/ca.21234
7. Zeiss J, Guilliam-Haidet L. MR demonstration of anomalous muscles about the volar aspect of the wrist and forearm. Clinical Imaging. 1996; 20 (3). Available from: https://doi.org/10.1016/0899-7071(95)00013-5
8. Peers SC, Kaplan FT. Flexor Carpi Radialis Brevis Muscle Presenting as a Painful Forearm Mass: Case Report. The Journal of Hand Surgery. 2008; 33 (10). Available from: https://doi.org/10.1016/j.jhsa.2008.06.014
9. Claassen H, Schmitt O, Schulze M, Wree A. Variation in the hypothenar muscles and its impact on ulnar tunnel syndrome. Surgical and Radiologic Anatomy. 2013; 35 (10). Available from: https://doi.org/10.1007/s00276-013-1113-5
10. Nellans K, Galdi B, Kim HM, Levine WN. Ulnar Neuropathy as a Result of Anconeus Epitrochlearis. Orthopedics. 2014; 37 (8). Available from: https://doi.org/10.3928/01477447-20140728-92
11. Li X, Dines JS, Gorman M, Limpisvasti O, Gambardella R, Yocum L. Anconeus Epitrochlearis as a Source of Medial Elbow Pain in Baseball Pitchers. Orthopedics. 2012; 35 (7). Available from: https://doi.org/10.3928/01477447-20120621-39
12. Bhashyam AR, Harper CM, Iorio ML. Reversed Palmaris Longus Muscle Causing Volar Forearm Pain and Ulnar Nerve Paresthesia. The Journal of Hand Surgery. 2017; 42 (4). Available from: https://doi.org/10.1016/j.jhsa.2016.11.016
13. Morgenstein A, Lourie G, Miller B. Anconeus epitrochlearis muscle causing dynamic cubital tunnel syndrome: a case series. Journal of Hand Surgery (European Volume). 2016; 41 (2). Available from: https://doi.org/10.1177/1753193414559491
14. Claassen H, Wree A. Multiple variations in the region of Mm. extensores carpi radialis longus and brevis. Annals of Anatomy - Anatomischer Anzeiger. 2002; 184 (5). Available from: https://doi.org/10.1016/s0940-9602(02)80084-x
15. Rao Mohandas KG, Venkata Ramana V, Bhat SM, Sreenivas B, Samuel VP, Pamidi N. Four cases of variations in the forearm extensor musculature in a study of hundred limbs and review of literature. Indian Journal of Plastic Surgery. 2006; 39 (02). Available from: https://doi.org/10.1055/s-0039-1699145
16. Nayak SR, Madhan Kumar SJ, Krishnamurthy A, Prabhu LV, Ranade AV, Rai R, et al. An additional radial wrist extensor and its clinical significance. Annals of Anatomy - Anatomischer Anzeiger. 2007; 189 (3). Available from: https://doi.org/10.1016/j.aanat.2006.10.005
17. Wood VE. The extensor carpi radialis intermedius tendon. The Journal of Hand Surgery. 1988; 13 (2). Available from: https://doi.org/10.1016/s0363-5023(88)80058-3
18. Smith J, Pourcho AM, Kakar S. Sonographic Appearance of the Extensor Carpi Radialis Intermedius Tendon. PM&R. 2015; 7 (7). Available from: https://doi.org/10.1016/j.pmrj.2015.04.005
19. Standring S, editor. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 41st ed. London: Elsevier; 2016. p. 84–108.
Copyright
©2026 (Hema) et al. This is an open-access journal, and articles are distributed under the terms of the Creative Commons Attribution License CC-BY 4.0. (https://creativecommons.org/licenses/by/4.0/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
Cite this article
Hema N, Gadade V, Kishve P, Srivatsa PS, Suhas R, Sharma P. Study of Anomalous Tendons of the Upper and Lower Limb Muscles and
their Clinical and Embryological Significance. Perspectives in Medical Research 2026; 14(1):4-8 DOI: 10.47799/pimr.1401.25.62