Volume: 13 Issue: 3
Effect of Anaesthesia – Electroconvulsive Therapy Time Interval on Duration of Convulsion - A Randomized, Open Labelled Comparative Study
Year: 2025, Page: 148-151, Doi: https://doi.org/10.47799/pimr.1303.25.48
Received: Aug. 2, 2025 Accepted: Oct. 25, 2025 Published: Dec. 30, 2025
Abstract
Introduction: Typical anaesthetic agents used during Electro Convulsive Therapy (ECT) have anticonvulsant effect which can impact the generalized seizure induced during the ECT procedure. As per the recent literature, Anaesthesia to ECT time interval (AETI) has significant impact on duration of convulsion and quality of seizure. Hence, the current study was aimed at assessing the AETI on duration of convulsion and its efficacy. Methodology: It is a randomized, comparative study. Subjects were randomized into two groups, Group A had longer AETI - 90 seconds, Group B shorter AETI of 30 seconds. Total 60 samples with 30 subjects in each group. All were given 4 sessions of ECTs, and the duration of seizure was measured after each session, clinical outcome was measured by Brief Psychiatric Rating Scale (BPRS) before and after the 4th session of ECT. Results: The mean duration of convulsion in Group A (45.97±12.57 seconds) is longer compared to Group B (23.69±5.86 seconds) and was statistically significant, even in individual sessions of ECT, group A had longer duration of convulsion. The mean decrease in BPRS scores of both groups were compared as a measure of efficacy and found that Group A had a higher mean decrease in BPRS score (9.53±3.05) compared to Group B (6.5±2.58) which was statistically significant. Conclusion: Study showed that Group A with longer AETI when compared to Group B with shorted AETI, had longer duration of convulsion and a good clinical outcome as measured with mean decrease in BPRS score, which were statistically significant.
Keywords: Anaesthesia - ECT time interval (AETI), Brief Psychiatric Rating Scale (BPRS), Clinical outcome, Duration of convulsion, Electroconvulsive therapy (ECT), Schizophrenia
INTRODUCTION
Electroconvulsive therapy (ECT) has proven to be a highly effective treatment for various psychiatric disorders, such as drug-resistant depression, schizophrenia, catatonia, and mania 1 . In this approach, the procedure is carried out while the patient is under general anesthesia, during which minor electrical currents are applied to the brain, intentionally inducing temporary seizures 2 . Different types of anesthetics are employed in electroconvulsive therapy, each with its own set of benefits and drawbacks. The administration of electrical stimulation during ECT induces seizures while the patient is under anesthesia 2 .
The anticonvulsant effects of the typical anaesthetic agents commonly employed for general anaesthesia in ECT can significantly influence the resulting generalised seizure 1 . The impact of these effects varies based on factors including the type of drugs administered, the level of anesthetics present in the brain during seizure initiation, and the dosage administered 2 . It has been shown that an increased anaesthetic dosage is linked to seizure threshold, requiring a greater charge to induce a seizure 1 , Additionally, there are indications that medications possessing anticonvulsant characteristics can impact the duration of seizures, and may also reduce the effectiveness of treatment 3 .
Research has primarily concentrated on the significance of the specific anaesthetic agent used during ECT or the exact dosage given. However, it is also crucial to take into account the levels of anaesthetic present in the blood and brain at the moment of administering the stimulus. Since unconsciousness is triggered by a rapid intravenous injection, it is logical to assume that the levels of anaesthetic in the plasma and brain will decrease after reaching a peak. Therefore, the timing of delivering the ECT stimulus concerning the levels of anaesthetic in the brain may play a vital role in reducing the anticonvulsant effects of anaesthesia on the effectiveness of ECT 4 . It is expected that the timing of the ECT stimulus administration plays a crucial role in determining ECT effectiveness, given that the blood plasma concentration decreases over time following the anaesthetic injection 1 .
Studies have demonstrated that the duration between administering the anesthetic and delivering the ECT stimulus has an impact on the strength and characteristics of the seizure induced by ECT. 1 Galvez et al. showcased in their study that extended intervals between anaesthesia and electroconvulsive therapy (ECT) resulted in enhanced seizure quality. This finding was observed in a retrospective analysis of 84 patients who underwent propofol anaesthesia 5 . Taylor and colleagues also showed in a recent randomized clinical trial that a longer interval between anesthesia and ECT leads to higher quality seizures induced by ECT 3 .
Moreover, it is worth considering whether a longer duration of convulsion or enhanced seizure quality truly translates to a superior outcome. After all, the ultimate objective of optimizing the anesthetic approach in electroconvulsive therapy (ECT) is to enhance clinical outcomes, specifically efficacy and cognition. The retrospective cohort study conducted by Xiao Wei Tan et al found that an extended AETI is linked to improved seizure quality and has a significant impact on cognition, similar to what would be anticipated with increased ECT dosing. However, the study did not establish a clear association with treatment effectiveness 1 .
It is imperative to emphasize the necessity for further research in the field of AETI and its impact on clinical outcomes or efficacy in clinical settings. Hence the current study is aimed at effect of time interval between anaesthesia to ECT induction time on the duration of convulsion and the outcome in the participants
Aims and Objectives:
This study aimed to identify the effect of Anaesthesia to ECT time interval (AETI) on duration of convulsion and clinical outcome in subjects with Schizophrenia
MATERIALS AND METHODS
This was a randomized comparative study conducted in a tertiary care psychiatry hospital after getting approval from the Institutional Ethics Committee. The subjects were selected from the pool of patients who were diagnosed with Schizophrenia and were posted for ECT as the modality of the treatment by the primary treating consultant. Schizophrenia subjects who were between 18 to 60 years, posted for ECT and gave written informed consent to participate in the study were included in the study and those with comorbidities like heart disease, intellectual disability and major neurological disorders were excluded from the study.
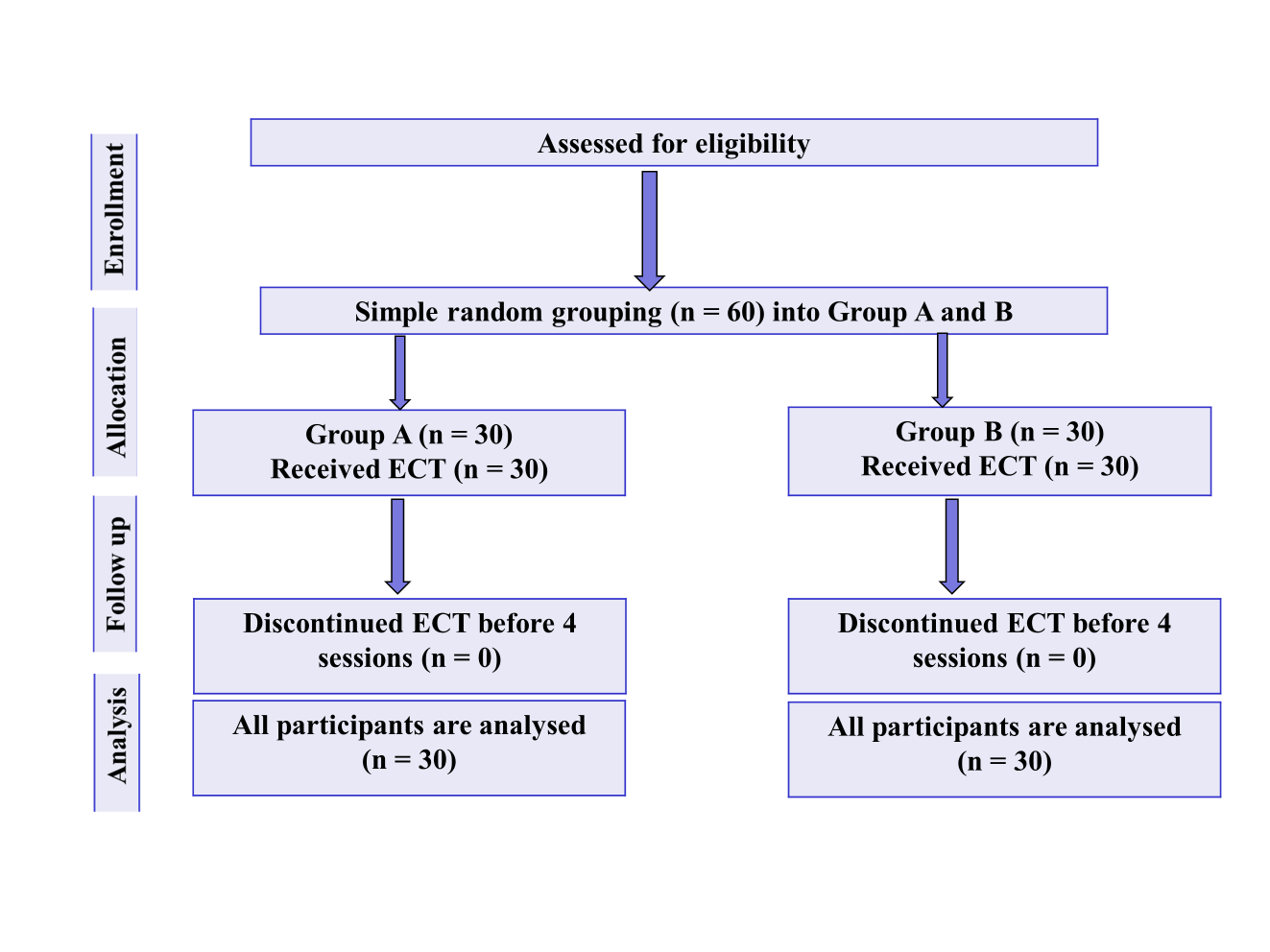
Anaesthesia to ECT time interval (AETI) was defined as the time interval from the time of injecting general anesthetic drug and induction of electrical stimulus. The study groups were named Group A and Group B with AETI as 90 seconds and 30 seconds respectively and all the subjects of both groups received four modified ECT sessions on alternate days as per the institution protocol. A total of 60 subjects meeting the inclusion and exclusion criteria were selected and randomized to two groups alternatively and allocation concealment was done.
Before the first ECT session, the sociodemographic and clinical data of all the subjects was collected. The severity of illness was rated using Brief Psychiatry Rating Scale (BPRS) at baseline and after the 4th session of ECT to determine the level of improvement.
The ECT sessions were conducted following the standard protocol and anaesthesia was induced with Propofol (0.75-1mg/kg body weight) as the inducing agent for all the subjects along with other necessary medication for general anaesthesia by the Anaesthetist. After induction, time was noted to give the electrical stimulus – 90 seconds for subjects in Group A and 30 seconds for subjects in Group B. The duration of convulsion was recorded by observing the external movement of upper limb using the cuff method. Statistical analysis was done using Statistical Package for Social Sciences (SPSS) software version 25.0.
RESULTS
Table 1: Socio-demographic profile
|
Variable |
Group A |
Group B |
|
Number of Subjects |
30 |
30 |
|
Gender |
|
|
|
Male |
16 (053.3%) |
19 (063.3%) |
|
Female |
14 (046.7%) |
11 (036.7%) |
|
Total |
30 (100.0%) |
30 (100.0%) |
|
Age (Mean ± SD) |
30.83 ± 4.99 |
30.66 ± 5.55 |
|
Education in years (Mean ± SD) |
10.12 ± 6.19 |
10.06 ± 6.13 |
|
Employment status |
|
|
|
Employed |
17 (056.7%) |
19 (063.3%) |
|
Unemployed |
13 (043.3%) |
11 (036.7%) |
|
Religion |
|
|
|
Hindu |
25 (083.3%) |
21 (070.0%) |
|
Christian |
05 (016.7%) |
07 (023.3%) |
|
Muslim |
00 (000.0%) |
02 (006.7%) |
|
Marital Status |
|
|
|
Married |
17 (056.7%) |
21 (070.0%) |
|
Unmarried |
07 (023.3%) |
05 (016.7%) |
|
Separated/Divorced |
06 (020.0%) |
04 (013.3%) |
|
Domicile |
|
|
|
Rural |
17 (056.7%) |
16 (053.3%) |
|
Urban |
13 (043.3%) |
14 (046.7%) |
|
Duration of illness |
6.73 ± 3.76 |
9.70 ± 5.97 |
In group A almost equal distribution of male and female and in group B male participants were more than female and no significant difference in age between both groups. In both groups majority of the population were employed. Group A had only Hindu and Christian population with majority of them belonging to Hindu religion and in Group B Hindu, Christian, Muslim participants were there with majority belonging to Hindu religion. Majority of the participants were married, and few participants were divorced/unmarried. Duration of illness in years was calculated, and mean duration was significantly higher in group B compared to group A.
Table 2: Duration of convulsion between the two groups in individual ECT sessions
|
|
Group A |
Group B |
Significance |
|
In 1st ECT (Mean±SD) |
51.3±15.84 |
27.5±8.08 |
<0.00001 |
|
In 2nd ECT (Mean±SD) |
47.0±02.96 |
25.0±4.41 |
<0.00001 |
|
In 3rd ECT (Mean±SD) |
43.1±10.45 |
21.8±3.10 |
<0.00001 |
|
in 4th ECT (Mean±SD) |
40.8±09.81 |
19.6±2.96 |
<0.00001 |
|
All 4 ECT sessions (Mean±SD) |
45.6±11.21 |
23.5±4.02 |
<0.00001 |
Duration of convulsion of each session in group A and group B was calculated and when compared group A had significantly higher mean than group B in all (1st , 2nd ,3rd, 4th sessions) sessions, and total mean of all 4 sessions in group A and group B were calculated and compared, it showed total mean of all 4 ECT session in Group A had significantly higher mean duration of convulsion compared to group B.
Table 3: Comparison of change in BPRS scores between the two groups
|
Variable |
Group A |
Group B |
P value |
|
Baseline BPRS score (Mean± SD) |
42.03±2.64 |
40.80±2.2 |
0.033 |
|
BPRS score after 4th ECT (Mean±SD) |
32.4±2.81 |
34.26±2.3 |
0.0059 |
|
Mean decrease in BPRS score from baseline (Mean±SD) |
9.53±3.05 |
6.5±2.58 |
<0.00063 |
Baseline symptoms in participants were assessed before 1st ECT session using BPRS and mean BPRS score in group A was higher than group B, and mean decrease in BPRS score was also significantly higher in group A, meaning group A with longer AETI of 90 seconds AETI had better clinical outcome compared to group B with shorter AETI of 30 seconds.
DISCUSSION
The purpose of this study was to find out the effect of AETI (anaesthesia - ECT time interval) on duration of convulsion and also the clinical outcome of the patient post ECT (measured using BPRS). In this study 60 participants of inpatients who were posted for ECT was taken and there were total 35 males and 25 females with an average of 30 years age and mean education years of 10 years and majority belonging to Hindu religion and the mean duration of illness in years was significantly higher in group B compared to group A.
Upon comparing group A with longer AETI (90secs) with group B with shorter AETI (30secs), the duration of convulsion was longer in group A compared to group B, indicating longer the time interval between anaesthesia and ECT induction which was done in group A resulted in longer duration of convulsion and the results were comparable to most of the previous studies Tan XW 1, Javadi AH et al 2 , Taylor 3, 4 , Galvez 5, Jorgensen A et al 6 and comparison was done on individual ECT session of the both group i.e. (1st ECT of group A vs 1st ECT of group B, so on.) and even on individual ECT session group A had significantly longer duration of convulsion compared to group B.
The clinical outcome in individual groups were also measured pre ECT and post 4th ECT using BPRS scale and the change/decrease in BPRS score was taken as improvement score. Mean change of BPRS SCORE was significantly higher in group A compared to group B, but group B participants had longer duration of illness compared to group A which could be a confounding factor.
Even though there was reduction in BPRS score, both group A and group B participants didn’t show full response - that is 50% reduction in BPRS score from the baseline, this could be because our study calculated the BPRS score after 4th ECT and not at the end of the ECT course, so some would have responded in further ECT sessions.
So, by the results group A with longer AETI had better duration of convulsion and better clinical outcome compared to the group B with shorter AETI and most of the previous studies didn’t measure the clinical response or outcome, in that aspect this is one of the few studies which did compare the effect of AETI on clinical outcome in participants with schizophrenia.
CONCLUSION
The main conclusion of this study is longer the time interval between anaesthesia to ECT induction, longer the duration of convulsion, which was also reflected in the better clinical outcome of the patients. So, it’s better to monitor the time interval between the anaesthesia to ECT induction time to have a longer duration of convulsion and thus the outcome.
LIMITATIONS
-
Our study was done using a participant size of around 60, so larger participant size would help in better understanding.
-
Side effects of ECT such as cognition weren’t noted in this study.
-
Assessment of outcomes after only 4 ECT limited the ability to fully explore associations between the AETI and clinical outcomes.
-
Also, multiple setting with heterogenous population would help in applying the results to the general population.
References
-
Tan, Xiao Wei, Tor, Phern Chern, Martin, Donel & Loo, Colleen . 2021. Association of Anaesthesia-ECT time interval with ECT clinical outcomes: A retrospective cohort study. Journal of Affective Disorders 285:58–62.
-
Javadi, Alireza Haji Seyed, Najafian, Ehsan, Kayalha, Hamid & Shafikhani, Ali Akbar . 2021. Evaluating Factors Affecting the Time Interval Between Propofol Injection and Induction of Electro-convulsion and Relationship Between These Factors and Duration of Convulsion. Anesthesiology and Pain Medicine 11(4):e117442.
-
Taylor, Rohan, Hadzi-Pavlovic, Dusan, Nikolin, Stevan, Bull, Michael, Wark, Harry, Leyden, John, Harper, Simon, Martin, Donel, Galvez, Veronica & Loo, Colleen . 2019. The anaesthetic-ECT time interval with thiopentone—Impact on seizure quality. Journal of Affective Disorders 252:135–140.
-
Taylor, Rohan, Wark, Harry, Leyden, John, Simpson, Brett, Mcgoldrick, Jenny, Hadzi-Pavlovic, Dusan, Han, Hank Ke, Nikolin, Stevan, Martin, Donel & Loo, Colleen . 2020. Effects of the Anaesthetic-ECT time interval and ventilation rate on seizure quality in electroconvulsive therapy: A prospective randomised trial. Brain Stimulation 13(2):450–456.
-
Gálvez, Verònica & Loo, Colleen K . 2017. Clinical Applicability of Monitoring the Time Interval Between Anesthesia and Electroconvulsive Therapy. The Journal of ECT 33:4–6.
-
Jorgensen, A, Christensen, S J, Jensen, A E K, Olsen, N V & Jorgensen, M B . 2018. The influence of the anesthesia-to-stimulation time interval on seizure quality parameters in electroconvulsive therapy. Journal of Affective Disorders 231:41–43.
Copyright
©2025 (Thanganagarasan) et al. This is an open-access journal, and articles are distributed under the terms of the Creative Commons Attribution License CC-BY 4.0. (https://creativecommons.org/licenses/by/4.0/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
Cite this article
Thanganagarasan T, Guyton A, Swathi P, Reddy PL. Effect of Anaesthesia – Electroconvulsive Therapy Time Interval on Duration of Convulsion - A Randomized, Open-Labelled Comparative Study. Perspectives in Medical Research. 2025;13(3):148-151 DOI:
10.47799/pimr.1303.25.48